12281360
Descripción
Fichas por Ashutosh Kumar, actualizado hace más de 1 año
|
|
Creado por Ashutosh Kumar
hace casi 7 años
|
|
| Pregunta | Respuesta |
| Dx: Etiology: Clinical features: Rx: | Pityriasis rosea Etiology: Viral Clinical features: Herald Patch: Single solitary, salmon-coloured patch. Fir tree: days to weeks after the herald patch a secondary rash appears mainly on the chest and back consisting of bilateral and symmetric macules with a distribution according to the skin tension lines, spreading outward from the midline like a christmas tree. Rx: Self limiting; resolves in 6-8 weeks. Treatment is supportive; treat dryness and pruritus Mnemonic: HER MOTHER SMOKES FIR TREE CIGARETTES Her: .Herald patch Mother: Mother patch Smokes: Secondary syphilis like lesion Fir tree: Christmas tree like arrangement Cigarette: Cigarette paper like scales |
| Dx: Etiology: Epidemiology: Clinical features: Diagnostic test: Rx: | Pityriasis versicolor Etiology: Yeast of malassezia genus. Microbe produces azelaic acid which inhibits melanin synthesis resulting in pigmentation of variable colour. Epidemiology: Affects people who perspire heavily (hot, humid climates or gyming). Clinical features: Affected skin darker in winter, lighter in summer (does not tan); versicolor (variable). Dx: Diagnosed clinically. Can do Wood lamp (black light) examination- yellow green fluorescence in affected areas. Rx: Topical antifungal |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Cellulitis: Etiology: Acute infection of full thickness skin and subcutaneous tissue.. Staph aureus or strep pyogenes. Clinical features: Pain, edema, erythema with indistinct borders +/- regional lymphadenopathy, systemic symptoms Lymphangitis (ascending infection) may occur; visible red streak going proximally. Dx: FBC and differentials Rx: Antibiotics |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Erysipelas Etiology: Superficial skin infection with upper dermis and lymphatics. GABS (strep pyogenes) almost always. Clinical features: Intense erythema, induration and sharply demarcated borders (differentiating from other skin disorders) Dx: FBC and differentials Rx: Penicillin or 1st generation cephalosporin (cefazolin or cephalexin) |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Impetigo: Etiology: Staph aureus or GABS. Clinical features: Acute purulent epidermis infection with vesicles progressing to golden yellow honey crusted lesions surrounded by erythema Common sites: Face, arms, legs and buttocks. Dx: Swab; gram stain and culture. Rx: Flucloxacillin |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: Sequelae: | Furuncles (boils): Etiology: S.aureus infection of hair follicle and subcutaneous tissue. Clinical features: Red, hot, tender inflammatory nodules with a central yellowish point, which forms over summit and ruptures. Dx: Clinical Rx: Incise and drain large furuncles to relieve pressure. Febrile/cellulitis: Culture blood, and aspirate fluid for gram stain and C&S. Flucloxacillin Sequelae: Can coalesce to form carbuncle (deep seat abscess formed by multiple furuncles) |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Erythema nodosum: Etiology: NODOSUMM NO cause (idiopathic) 40% cases Drugs Other infections (Rheumatic fever) Sarcoidosis UC and Crohn’s Malignancy Many infections Clinical features: Acute or chronic inflammation of subcutaneous fat (panniculitis) Round, red, tender poorly demarcated nodules Associated arthralgia, fever and malaise Sites: Asymmetrically on extensor lower legs, knees and arms (typically shins) Dx: CXR (sarcoidosis and chest infection) Throat culture, Anti-streptolysin O antibody titre, PPD TB skin test. Rx: Treat underlying cause Symptomatic: Bed rest, compressive bandages, wet dressings, NSAIDS, intralesional steroids |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Molluscum contagiosum: Epidemiology: Young children and sexually active young adults Etiology: Pox virus Direct contract, auto inoculation and sexual contact Clinical features: Discrete umbilicated vesicles Dx: Clinical diagnosis although biopsy can be performed Rx: Self-limiting, can 1-2 years to resolve. |
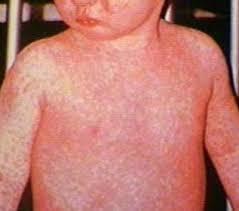
| Dx: Etiology: Clinical features: Diagnostic test: Rx: Prevention: | Measles: Etiology: Morbillivirus Airborne transmission Clinical features: Infectious 4 days before rash and up to seven days after. Prodrome of cough, coryza and conjunctivitis (3 C’s) Enanthem (rash or spot on mucous membrane): Koplick spots 1-2 days before rash Morbilliform rash: Rash comprised of both macules and papules starting at the hairline and moving downwards whilst sparing the limbs Dx: Clinical Serology: IgM measles Rx: Supportive (antihistamines, calamine lotion, bed rest) Contacts: Immunization within 72 hrs of exposure or IgG within 6 days of exposure Report to public health Prevention: MMR vaccine Mnemonic: 7 C’s Cough Coryza Conjunctivitis Concurrent fever and rash Koplik Cephalocaudal spreading rash Cervical lymphadenopathy |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: Sequelae: | Herpes Zoster (shingles): Etiology: Reactivation of varicella zoster virus (VZV) Risk factors for reactivation include old age and immunosuppression Clinical features: Herpetiform dermatomal vesicular rash comprised of multiple vesicles, bullae and pustules, confluent in some areas with ulceration and surrounding erythema. Involves single dermatome and rarely crosses midline. Dx: Clinical Rx: Compress with normal saline, Burrow’s or betadine solution. Analgesia (NSAID or amitriptyline) Acyclovir (must initiate within 72 hrs to be of effect) Gabapentin 300-600 mg PO tid for post Herpetic neuralgia Sequelae: Hutchinson’s sign: Shingles on the tip of the nose suggests nasociliary branch of V1/ophthalmic branch of trigeminal is involved and so could affect the optic nerve. Ramsay Hunt syndrome: facial nerve involvement Ophthalmic nerve reactivation: HSV keratitis Post-Herpetic neuralgia |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: Prevention: | Chicken pox: Epidemiology: Children under 10 Once had, confers lifelong immunity Etiology: Primary infection with varicella zoster virus Highly infectious with airborne spread Clinical features: Begins as itchy red papules progressing to vesicles + constitutional symptoms Adults: Prodromal phase for 48 hrs; more serious than in children and can be life-threatening. Dx: Clinical PCR of swab of skin lesions Serology in pregnant women Rx: Itching: Calamine lotion and antihistamines. Fever: Paracetamol (NOT ASPIRIN: REYE’S syndrome) Contagious 1-2 days before rash appears and 5-10 days until all blisters have formed scabs; stay at home. Immunocompromised: IV acyclovir Prevention: Immunization |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Rubella: Etiology: Rubivirus Droplet transmission Clinical features: Prodrome of low grade fever Pink maculopapular rash STAR complex: Sore throat, arthralgia, rash Dx: Clinical Serology for IgM against Rubella Rx: Supportive Report to public health Vaccine for non immune contacts Caution to pregnant woman with exposure |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Erythema infectiosum (slap cheek): Etiology: Parvovirus B19 (erythrovirus) Clinical features: Uniform, erythematous maculopapular rash affecting bilateral cheeks and possibly trunk 10-17 days after symptoms of flu Dx: Clinical Serology and PCR available. Rx: Supportive |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Hand, foot and mouth: Etiology: Enterovirus (Coxsackie virus) Spread via direct and indirect contact via bodily fluids Clinical features: Hand, foot and mouth distribution of vesicle and pustules on an erythematous base Dx: Clinical Rx: Supportive; Do not pop blisters to enable containment of contagion, dressings, fluids (IV fluids indicated if painful to drink). |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Roseola infantum: Etiology: HHV-6 Clinical features: High grade fever 3-5 days which subsides to give rise to a pink, blanching maculopapular rash starting at the neck and trunk then spreading to face and extremities. Dx: Clinical Rx: Supportive Risk of febrile seizures; reassure benign |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Scabies Etiology: Scabies mite Clinical features: Red, excoriated papules, nodules with burrows in web spaces and folds, very pruritic Dx: Clinical Microscopic examination of burrows Rx: Permethrin cream 2x applications, 1 week apart Wash clothes and bed sheets Rx family members Pruritus will persist for 1-2 weeks |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Atopic dermatitis Etiology: Allergy to something Clinical features: Acute: Vesicles papules Subacute: Crusting, excoriation Chronic: Lichenification, fissuring, xerosis Pruritus results in skin breakage resulting in further exposure to irritant resulting in more eczema Dx: Clinical Allergy testing Rx: Moisturizers, emollients, topical corticosteroids |
| Dx: Etiology: Clinical features: Diagnostic test: Rx: | Irritant/contact dermatitis Etiology: Irritation Clinical features: Poorly demarcated pruritic erythematous rash Dx: Clinical Rx: Eliminate contact with irritant and use of topical barriers or in severe cases short term topical steroids. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.