4729471
| Question | Answer |
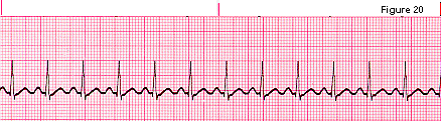
| ] | NORMAL SINUS RHYTHM rate: 60-100 bpm rhythm: regular pacemaker: SA node P wave: same morphology (shape & size) PR interval: normal (0.12-0.20) QRS Complex: Normal (</= 0.10) P to QRS Ratio: 1:1 treatment: none |
| SINUS BRADYCARDIA rate: <60 BEATS/MIN Rhythm: Regular Pacemaker: SA Node P Wave: Same Morphology PR Interval: Normal QRS Complex: Normal P to QRS Ratio: 1:1 | |
| Sinus Bradycardia etiology | Normal in well-conditioned athletes and w/ sleep increased vagal tone/ excessive vagal stimulation inferior wall MI meds (Digoxin or beta-blockers) electrolyte imbalances (hyperkalemia) S/S of hypofusion: ACLS: meds- atropine sulfate (increase rate and contractility of heart Emergency cardiac pacing (trancutaneous) |
| SINUS TACHYCARDIA Rate: >100 BEATS/MIN (usual 160 upper limit) Rhythm: Regular Pacemaker: SA Node P Wave: Same Morphology PR Interval: Normal QRS Complex: Normal P to QRS Ratio: 1:1 | |
| Sinus Tachycardia etiology | Caffeine, alcohol, and/or nicotine ingestion exercise fever pain/anxiety hypovolemia (not enough O2) MI hyperthyroidism Treatment: correct/treat underlying cause symptomatic: beta-blocker may be used for rate control; Metroprolol (Lopressor) for sustained tach |
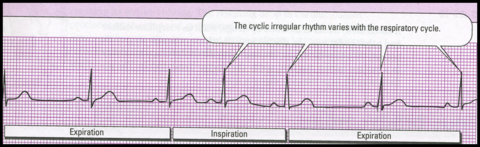
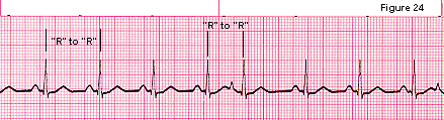
| SINUS ARRYTHMIA rate: 60-100 bpm rhythm: SLIGHTLY IRREG; RESP VARIATION: INCREASAED RATE INSPIRA, DECREASED RATE ON EXPIRATION Pacemaker: SA Node PR Interval: Normal QRS Complex: Normal P to QRS Ratio: 1:1 Treatment: Usually None | |
| PREMATURE ATRIAL COMPLEX (PAC) rate: depends on underlying rhythm RHYTHM: IRREG DUE TO EARLY COMPLEX pacemaker: early complex - ectopic atrial focus P WAVE: EARLY CMPLEX WITH DIFFERENT MORPHOLOGY PR interval: normal; early complex may be different QRS complex: normal P to QRS Ratio: 1:1 | |
| Premature Atrial Complex (PAC) etiology | caffeine, alcohol, and/or nicotine ingestion stress/anxiety mitral valve prolapse heart failure Treatment: not usually necessary unless frequent (> 6 PACs /min) then treatment focused on underlying cause teach to manage stress and avoid caffeine, alcohol, and/or nicotine |
| ATRIAL FLUTTER RATE: (ATRIAL) 250-400 BPM & (VENTRICULAR) 60-150 BPM RHYTHM: BOTH ATRIAL & VENTRICLAR Pacemaker: ectopic atrial focus P WAVE: "SAWTOOTH" PATTERN (F WAVES) PR interval: difficult to determine QRS complex: normal P to QRS ratio: 2:1, 3:1, 4:1 | |
| ATRIAL FIBRILLATION (A-FIB) RATE: (ATRIAL) 400-600 BPM & VENTRICULAR 40-250 BPM RHYTHM: BOTH ATRIAL & VENTRICULAR IRREG pacemaker: numerous ectopic atrial foci P WAVE: NO IDENTIFIABLE P WAVES PR interval: unable to determine (UTD) QRS complex: normal P to QRS ratio: many:1 | |
| A fib/flutter etiology | Coronary artery disease value disorders heart failure cardiac surgery COPD ACLS Treatment: meds for rate control - calcium-channel blocker (diltiazem), beta-blocker or Digoxin Cardioversion: anticoagulation if present > 48 hours pharmacologic: amiodarone (cordarone), ibutilide (Corvert) electrical: synchrinized cardioversion / overdrive pacing Longer term: anticoagulation/radiofrequency ablation risk - prevent clot formation! proximal - in and out of AFIB |
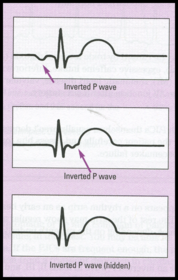
| PREMATURE JUNCTIONAL COMPLEX (PJC) rate: depends on underlying rhythm RHYTHM: IRREG - DUE TO EARLY COMPLEX pacemaker: early beat - ectopic junctional focus P WAVE: ABSENT (OBSCURED BY QRS) INVERTED BEFORE OR AFTER QRS COMPLEX PR interval: normal, early complex diff QRS complex: normal P to QRS Ratio: 0:1 or 1:1 (early complexes) | |
| Premature Junctional Complex (PJC) etiology | caffeine, alcohol, and/or nicotine ingestion Digoxin toxicity heart failure coronary artery disease AV node dysfxn Treatment: none - unless frequent, then focused on underlying cause |
| JUNCTIONAL ESCAPE RHYTHM RATE: 40-60 BPM (intrinsic rate of AV node) Rhythm: reg pacemaker: AV junction P WAVE: ABSENT (OBSCURED BY QRS); INVERTED BEFORE OR AFTER QRS COMPLEX PR interval: normal or UTD QRS complex: normal P to QRS ratio: 0:1 (absent) or 1:1 (inverted) | |
| Junctional Escape Rhythm etiology | vagal stimulation inferior wall MI heart failure valvular heart disease Digoxin toxicity Treatment: hemodynamically stable: treat the cause S/S of hypoperfusion ACLS: med - atropine sulfate Emergency cardiac pacing (transcutaneous) |
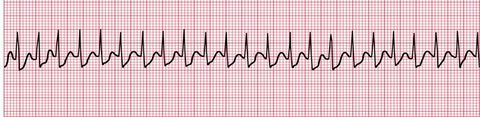
| SUPRAVENTRICULAR TACHYCARDIA (non-ventricular dysrhythmia) RATE: 150-250 BPM rhythm: reg P WAVE: DIFFICAUL TO INDENTIFY IF PRESENT; HIDDEN IN T WAVE pacemaker: ectopic atrial focus or junctional focus PR interval: normal QRS complex: usually normal P to qRS ratio: difficult to determine **SVT w/ sudden onset and cessation is termed "paroxysmal" | |
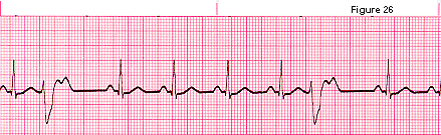
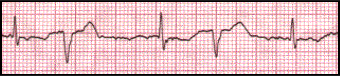
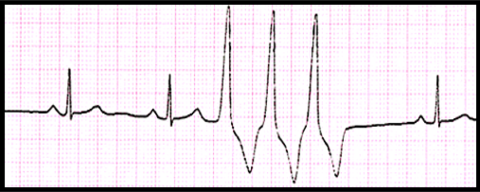
| PREMATURE VENTRICULAR COMPLEX (PVC) Rate: depends on underlying rhythm RHYTHM: IRREG - DUE TO EARLY COMPLEX pacemaker: early complex - ectopic ventricular focus P WAVE: ABSENT IN EARLY COMPLEX PR interval: normal; early compllexes may be different QRS COMPLEX: >.10 sec (EARLY, WIDE &BIZARRE) P to QRS ratio: 0:1 (early complexes) | |
| PVC configuartions Trigeminy | PVC every third beat |
| PVC Configurations Bigeminy | PVC every other beat |
| PVC Configurations Couplet Pair | Two PVCs in a row |
| PVC Configurations Triplet | Three PVCs in a row "Run of V-tach" most dangerous** |
| PVC Configuration Unifocal PVC | PVCs are identical (same shape) |
| PVC configuration multifocal PVC | PVCs with different shapes; more |
| PVC: more dangers | R on T phenomenon The superimposition of an ectopic beat on the peak of the proceeding T wave, which could result in ventricular tachycardia or ventricular fibrillation |
| Premature Ventricular Complexes etiology | Cardiac ischemia or infarction heart failure acid-base imbalances (hypokalemia) stimulant drugs (caffeine, alcohol, or nicotine) Treatment: rarely used unless PVCs are freq, pt is symptomatic or has dangerous forms of PVCs Teach to avoid stress and stimulants If treated: underlying cause is focus. meds - Sotalol (betapace), aminodarone (cardarone) or procainamide (Pronestyl) |
| VENTRICULAR ESCAPE RHYTHM RATE: VENTRICULAR = 20-40 BPM rhythm: reg paccemaker: purkinje fibers P WAVE: NONE PR interval: UTD QRS COMPLEX: > .10 SEC (WIDE AND BIZARRE) P to QRS ratio: UTD | |
| Ventricular escape rhythm etiology | myocardial ischemia or infarction Digoxin toxicity pacemaker failure metabolic imbalances Treatment: goal is to increase heart rate meds - Atropine or isoproterenol (Isuprel) Emergency cardiac pacing (transQ) |
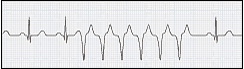
| VENTRICULAR TACHYCARDIA (VT) RATE: >100 BPM rhythm: reg pacemaker: ectopic ventricular focus P wave: none PR interval: UTD QRS COMPLEX: > .10 SEC (WIDE AND BIZARRE) P to QRS Ratio: UTD | |
| Ventricular tachycardia (VT) etiology | myocardial ischemia or infarction CAD valvular heart disease (MVP) heart failure cardiomyopathy electrolyte imbalances (hypokalemia) drug toxicity (digoxin or cocaine) pulmonary embolism rheumatic heart disease |
| VT Treatment | Hemodynamically stable: ACLS: Meds - sotalol (betapace), aminodarone (Cardarone) or procainamide (Pronestyl); Lidocaine 2nd line drug - synchronized cardioversion Hemodynamically unstable: ACLS: + pulse: synchronized cardioversion: start w/ 100J -> 200J -> 300J -> 360J -pulse: (treated like V-FIB); defibrillate ASAP - start w/ 360J If defibrillator unavail, perform CPR UNTIL defib avail |
| COARSE "early" VENTRICULAR FIBRILLATION (VF) RATE: >300 BPM RHYTHM: EXTREMELY IRREG pacemaker: ectopic ventricular foci p wave: none QRS complex: undulations; no identifiable QRS P to QRS Ratio: UTD | |
| FINE "late" V FIB RATE: >300 BPM RHYTHM: EXTREMELY IRREG pacemaker: ectopic ventricular foci p wave: none QRS complex: undulations; no identifiable QRS P to QRS Ratio: UTD | |
| Ventricular Fibrillation (VF) etiology | Myocardial ischemia or infarction valvular heart disease heart failure cardiomyopathy acid-base imbalances (hypokalemia) drug toxicity (digoxin, quinidine, or cocaine) unsuccessful treatment of VT Treatment: defibrillate ASAP - START W/ 360 J, perform CPR until avail if not |
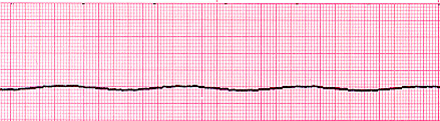
| ASYSTOLE: VENTRICULAR STANDSTILL RATE: NONE RHYTHM: NONE PACEMAKER: NONE P WAVE: NONE QRS COMPLEX: NONE P TO QRS RATIO: NONE Treatment (ACLS): immediate CPR; med - epinephrine, emergency cardiac pacing (transQ), treat or remove underlying cause | |
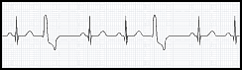
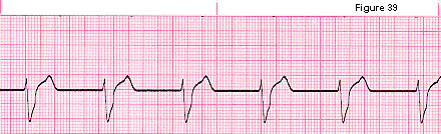
| FIRST DEGREE AV BLOCK Rate/Rhythm: depends on underlying rhythm P wave: same morphology Pacemaker: Block (delay) through AV node PR INTERVAL: PROLONGED > .20 & CONSTANT QRS complex: usually normal P to QRS Ratio: 1:1 | |
| SECOND DEGREE AV BLOCK: MOBITZ TYPE 1/ WENCKEBACH Rate/rhythm: depends on underlying rhythm P wave: same morphology; intermittently not conducted Pacemaker: block at AV node PR INTERVAL: PROGRESSIVELY INCREASES UNTIL A P WAVE APPEARS WITHOUT A QRS COMPLEX; "LONG, LONGER, DROP" QRS complex: usually normal P to QRS Ratio: more p waves than QRS complexes | |
| SECOND DEGREE AV BLOCK: MOBITZ TYPE II Rate/Rhythm: depends on underlying rhythm P wave: same morphology; intermittently not conducted pacmaker: block below the AV node PR INTERVAL: WHEN PRESENT CONSTANT; MAY BE PROLONGED QRS complex: usually normal P to QRS RATIO: MORE P WAVES THAN QRS COMPLEXES | |
| THIRD DEGREE AV BLOCK/ COMPLETE HEART BLOCK Rate: depends on underlying rhythm; atrial rate faster than ventricular rate Rhythm: depends on underlying rhythm P wave: same morphology; intermittently not conducted pacemakerL two seperate impulses atria & ventricle PR INTERVAL: VERY IRREG QRS complex: usually abnormal P TO QRS RATIO: NO RELATIONSHIP BETWEEN P WAVES & QRS COMPLEXES; MORE P WAVES THAN QRS COMPLEXES | |
| AV Blocks Treatment | First degree AV block & second degree type 1 -correct underlying cause (if poss) -close ECG monitoring Second Type II & third degree AV block -correct underlying cause (if poss) -close ECG monitoring -Temporary cardiac pacing (transQ) long-term: permanent pacemaker |
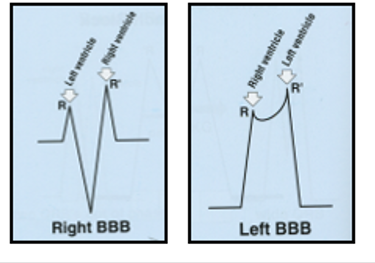
| VENTRICULAR CONDUCTION BLOCKS BUNDLE BRANCH BLOCK (BBB) cause by a block of conduction in the R or L bundle branch. result = delayed depolarization of the respective ventricle EKG: Wide QRS complex |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.