7878780
Description

Flashcards by RadTech Fairy, updated more than 1 year ago
|
|
Created by RadTech Fairy
about 8 years ago
|
|
| Question | Answer |
| Upper extremity usually uses _____ -scale contrast. | SHORT SCALE CONTRAST high contrast low kVp |
| What will happen when the part is not parallel to the IR? | SHAPE DISTORTION foreshortening elongation joint spaces closed |
| Oblique Digit | finger not parallel to IR *should be more concave to one side* |
| Oblique Digit | finger not obliqued to 45 degrees - can't see the concavity of one side of the digit joint spaces closed |
| Lateral Digit | finger bent back - not truly lateral |
| Lateral Digit | artifact |
| AP Thumb | metacarpals overlapping thumb |
| Oblique Thumb | slightly overrotated foreshortened distal phalanx |
| Lateral Thumbs | should be concave to one side only and straight on the other images are not truly lateral |
| PA Hand | distal phalynxes are bent flatten hand to true PA *should be equal concavity on all digits* |
| PA Hand | obliqued - fingers are not equally concave on both sides distal metacarpals are overlapped |
| Oblique Hand | Overly obliqued - metacarpals superimposed joint spaces closed - fingers bent |
| Oblique Hand | MCP joints superimposed - fingers too close together *underexposed |
| Oblique Hand | joint spaces closed hand overly obliqued MCP joints superimposed |
| Fan Lateral Hand | phalanges are superimposed and not well visualized patient's hand is externally rotated |
| Fan Lateral | patient's 2nd digit is bent - closed joint space hand is internally rotated |
| Fan Lateral | patient's metacarpals are not superimposed - hand is externally rotated distal phalanx's are bent - joint spaces closed not truly lateral |
| PA Wrist | wrist externally rotated - joint spaces closed, proximal metacarpals superimposed, carpals superimposed radiocarpal joint is closed |
| Oblique Wrist | over rotation radial styloid is not seen in profile |
| Lateral Wrist | under rotation - radius and ulna are not superimposed, hand is internally rotated |
| AP Forearm | not AP - wrist is internally rotated, proximal radius and ulna are superimposed |
| Lateral Forearm | Elbow is not 90 degrees proximal radius and ulna are superimposed |
| AP Elbow | humerus is externally rotated because the epicondyles are not in profile |
| AP Oblique Elbow Internal Rotation | Insufficient obliquity |
| AP Oblique Elbow Internal Rotation | Excessive obliquity |
| AP Oblique Elbow External Rotation | forearm is not parallel to IR capitulum-radial joint is closed olecranon is not in the fossa |
| AP Oblique Elbow External Rotation | Underrotation distal forearm slightly elevated |
| AP Oblique Elbow External Rotation | Overrotation |
| Lateral Elbow | The elbow is elevated above the level of the shoulder radial head anterior to coronoid - should be superimposed capitulum too proximal to trochlea radial tuberosity seen - hand is pronated |
| Lateral Elbow | Elbow is depressed below the level of the shoulder radial head superimposed by coronoid capitulum too distal to medial trochlea |
| Lateral Elbow | the distal wrist is elevated hand is pronated because you can see the radial tuberosity - should not see that |
| AP Humerus | humeral epicodyles not in profile radial head, neck and tuberosity to not superimpose ulna arm is externally rotated (greater tubercle in profile) |
| Lateral Humerus | over rotation places the humeral head within the field of the chest |
| Lateral Humerus | epicondyles are not perpendicular humerus is internally rotated (lesser tubercle is in profile medially) overrotation |
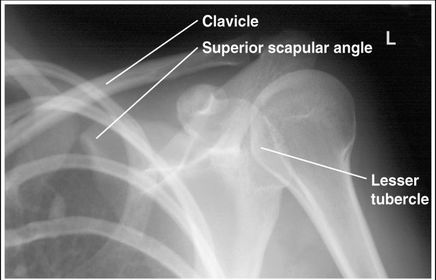
| AP Shoulder internal rotation | the MCP is tilted posteriorly as marked by the superior scapular angle is inferior to the clavicle |
| AP Shoulder | patient is rotated towards the unaffected shoulder: decreased thoracic superimposition over the scapular body |
| AP Shoulder | patient is rotated towards affected side:increased thoracic superimposition over the scapular body |
| Inferosuperior Axiolateral Shoulder | humerus is foreshortened - humeral head is distorted arm is not abducted 90 degrees from body |
| Grashey | Insufficient obliquity |
| Grashey | Excessive obliquity |
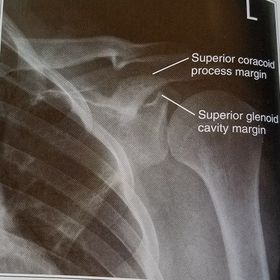
| Grashey | MCP is tilted posteriorly |
| PA Oblique Scapular Y-Lateral | Excessive Obliquity |
| PA Oblique Scapular Y-Lateral | Insufficient Obliquity |
| PA Oblique Scapular Y-Lateral | MCP is tilted anteriorly |
| PA Oblique Scapular Y-Lateral | MCP is tilted posteriorly |
| AP Clavicle | MCP is tilted anteriorly |
| AP Clavicle | MCP is tilted posteriorly |
| AP Clavicle | Patient is rotated towards affected shoulder |
| AP Clavicle | Patient is rotated towards unaffected shoulder |
| AP AC Joints Unilateral | MCP tilted anteriorly |
| AP Scapula | arm is not abducted so scapula is hidden behind the thorax |
| Lateral Scapula | Insufficient obliquity |
| Lateral Scapula | Excessive Obliquity |
| Oblique Sternum | projection taken as LAO instead of RAO sternum is projected within the heart and scapula |
| RAO Sternum | inadequate breathing technique |
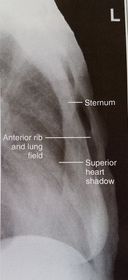
| Lateral Sternum | patient's left thorax is rotated anteriorly |
| Lateral Sternum | patient's right thorax is rotated anteriorly |
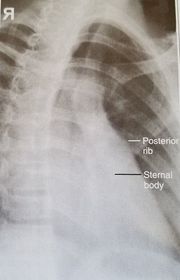
| PA Ribs Above Diaphragm Unilateral | patient rotated towards the right |
| PA Ribs Below Diaphragm Unilateral | Excessive obliquity |
| AP - LPO Ribs Above Diaphragm Unilateral | Insufficient obliquity |
| Left thorax is more anterior | |
| Right thorax is more anterior | |
| What's the evaluation criteria for the PA Finger X-Ray? | ANATOMY: distal phalynx -> distal 1/2 of metacarpal demonstrated CRITERIA: - equal concavity on both sides of phalanges - IP and MCP open - no overlapping of adjacent fingers POSITIONING: CR perpendicular @ PIP joint |
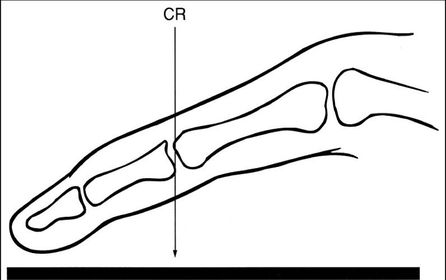
| What's the evaluation criteria for the Lateral finger x-ray? | ANATOMY: entire digit demonstrated CRITERIA: open joint spaces concave to one side, while the dorsal side is straight no overlapping of adjacent fingers/soft tissues POSITIONING: CR perpendicular @ PIP joint |
| Oblique finger x-ray image criteria? | ANATOMY: entire digit demonstrated CRITERIA: more concavity to one side open joint spaces no superimposition of adjacent fingers POSITIONING: CR perpendicular @ PIP joint |
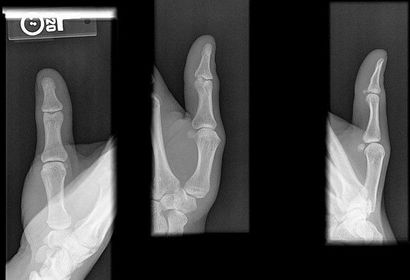
| AP Thumb Criteria | ANATOMY: entire digit including trapezium CRITERIA: equal concavity on both sides of digit open joint spaces no superimposition from adjacent bones POSITIONING: CR perpendicular @ 1st MCP joint |
| Oblique Thumb | ANATOMY: entire digit including trapezium CRITERIA: more concave to the side farthest from IR open joint spaces no superimposition from adjacent bones POSITIONING: CR perpendicular @ 1st MCP joint |
| Lateral Thumb | ANATOMY: entire digit including trapezium CRITERIA: most concave to one side, while the other is straight open joint spaces no superimposition from adjacent bones POSITIONING: CR perpendicular @ 1st MCP joint |
| PA Hand | ANATOMY: entire hand including 1'' of distal radius and ulna CRITERIA: equal concavity on either side of digits digits separated with no superimposition open joint spaces POSITIONING: CR perpendicular @ 3rd MCP joint |
| Oblique Hand | ANATOMY: entire hand including 1'' of distal radius and ulna CRITERIA: digits more concave to one side minimal overlap of 3rd-5th metacarpal shafts separation of the 2nd and 3rd metacarpals POSITIONING: CR perpendicular @ 3rd MCP joint |
| Lateral Hand | ANATOMY: entire hand including distal 1'' of radius and ulna superimposed CRITERIA: metacarpals and distal radius/ulna are superimposed thumb is free of superimposition *thumb in lateral position* open joint spaces POSITIONING: CR perpendicular @ 3rd MCP joint LAT Extension: foreign body localization LAT Flexion: phalanges |
| PA Wrist | ANATOMY: all carpals including midmetacarpals and distal radius/ulna CRITERIA: true PA is marked by symmetry of proximal metacarpals carpals should be free of superimposition of the metacarpals and radius/ulna POSITIONING: CR perpendicular @ midcarpals |
| Oblique Wrist | ANATOMY: carpals on lateral side of wrist, scaphoid CRITERIA: scaphoid well demonstrated 45 degree obliquity POSITIONING: CR perpendicular @ midcarpals |
| L | CRITERIA: radius/ulna should be superimposed thumb should be forward metacarpals superimposed POSITIONING: CR perpendicular @ midcarpals |
| AP Forearm | ANATOMY: entire forearm: wrist joint -> elbow joint CRITERIA: slight superimposition of proximal radius/ulna POSITIONING: CR perpendicular @ midforearm |
| Lateral Forearm | ANATOMY: entire forearm including wrist joint and elbow joint CRITERIA: humeral epicondyles must be superimposed distal radius/ulna superimposed half of radial head superimposed by coronoid process olecranon process in profile POSITIONING: CR perpendicular @ midforearm |
| AP Elbow | ANATOMY: distal humerus - proximal forearm CRITERIA: slight superimposition of proximal radius/ulna humeral epicondyles in profile open joint space POSITIONING: CR perpendicular @ midelbow |
| Medial Oblique Elbow | ANATOMY: proximal radius/ulna, distal humerus, medial epicondyle and trochlea CRITERIA: coronoid process in profile radial head and neck should superimpose the ulna olecranon process seen within olecranon fossa POSITIONING: CR perpendicular @ midelbow |
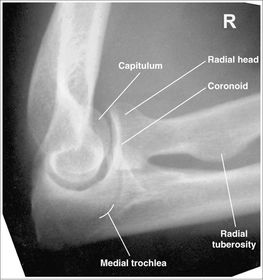
| Lateral Oblique Elbow | ANATOMY: open joint space, radial head, neck, tuberosity, and capitulum CRITERIA: radial head, neck, and tuberosity are free of superimposition humeral epicondyles and capitulum in profile POSITIONING: CR perpendicular @ midelbow |
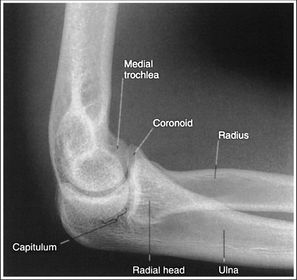
| Lateral Elbow Evaluation Criteria | ANATOMY: distal humerus, proximal forearm, entire elbow joint CRITERIA: humeral epicondyles are superimposed radial tuberosity is invisible (if visible the hand is pronated) half of the radial head superimposed by coronoid process Elbow is flexed 90 degrees to see/not see fad pads 3 concentric arcs visible POSITIONING: CR perpendicular @ lateral epicondyle |
| AP Humerus | ANATOMY: entire humerus: shoulder -> elbow CRITERIA: greater tubercle in profile - hand externally rotated humeral epicondyles are parallel to IR POSITIONING: CR perpendicular @ midhumerus |
| Lateral Humerus | ANATOMY: entire humerus: shoulder -> elbow CRITERIA: lesser tubercle in profile - arm internally rotated epicondyles superimposed POSITIONING: pt rotated 15-20 degrees from PA to get arm lateral and away from chest - flex elbow 90 degrees CR perpendicular @ midhumerus |
| AP Shoulder Neutral | ANATOMY: proximal humerus, lateral 2/3 of clavicle, open shoulder joint CRITERIA: humeral epicondyles are 45 degrees to the IR neither tubercle should be seen on the humeral head POSITIONING: CR perpendicular @ 1'' inferior to coracoid process |
| AP Shoulder Internal Rotation | CRITERIA: lesser tubercle in profile medially POSITIONING: CR perpendicular @ 1'' inferior to coracoid process |
| AP Shoulder External Rotation | CRITERIA: greater tubercle in profile laterally POSITIONING: CR perpendicular @ 1'' inferior to coracoid process |
| Scapular Y-Lateral | ANATOMY: humeral head resting in the 'Y' of the acromion and coracoid process CRITERIA: vertebral border and lateral border of scapula are directly superimposed humeral head is aligned with body of scapula POSITIONING: pt's unaffected arm is abducted 90 degrees, pt in 45-60 degree anterior oblique CR perpendicular @ scapulohumeral joint (neer) CR angled 10-15 degrees caudal @ scapulohumeral joint |
| Inferosuperior Axial Shoulder | ANATOMY: lateral view of the proximal humerus in relation to the glenoid fossa CRITERIA: lesser tubercle in profile medially humeral head is in the center of VOI POSITIONING: affected arm abducted 90 degrees, hand rotated externally with hand supinated CR horizontal 25-30 degrees medial to the scapulohumeral joint |
| Posterior Oblique Grashey | ANATOMY: glenoid cavity in profile glenohumeral joint center of VOI CRITERIA: open glenoid cavity anterior/posterior rims of glenoid cavity are superimposed POSITIONING: pt in 35-40 degree posterior oblique CR perpendicular @ glenoid cavity |
| AP Clavicle | ANATOMY: entire clavicle with both AC and SC joints included CRITERIA: entire clavicle and acromion are included lateral clavicle bows up, while the medial clavicle is superimposed by ribs 2-3 POSITIONING: CR perpendicular @ midclavicle |
| AP Axial Clavicle | ANATOMY: entire clavicle and both joints included CRITERIA: clavicle is more horizontal, and projected above the scapula and ribs medial end may be superimposed by ribs POSITIONING: CR angled 15-30 degrees cephalic @ midclavicle |
| AC Joints | ANATOMY: Bilateral AC joints included and open CRITERIA: non weight bearing and weight bearing projections marked correctly both joints included lateral clavicle almost horizontal POSITIONING: CR perpendicular @ jugular notch |
| AP Scapula | ANATOMY: entire scapula midscapula center of VOI CRITERIA: lateral border seen without superimposition of thorax humerus abducted 90 degrees POSITIONING: CR perpendicular @ midscapula |
| Lateral Scapula | ANATOMY: entire scapula CRITERIA: vertebral border and lateral border directly superimposed humerus abducted to view scapular body POSITIONING: 45-60 degree oblique (to get scapula perpendicular to IR) CR perpendicular to midscapular body |
| RAO Sternum | ANATOMY: jugular notch, SC joints, sternal body, and xiphoid process CRITERIA: sternum projected within heart shadow next to vertebral column POSITIONING: pt. rotated 15-20 degrees breathing technique CR perpendicular @ midsternum (2 fingers off downside spine) |
| Lateral Sternum | ANATOMY: manubrium, sternal body, and xiphoid in profile CRITERIA: 72'' SID reduces OID arms must be behind pt's back POSITIONING: CR perpendicular @ midsternum |
| AP/PA Ribs | ANATOMY: all ribs demonstrated 1-9 for upper 8-12 for lower CRITERIA: no motion/breathing POSITIONING: AP ribs when pt c/o posterior pain PA ribs when pt c/o anterior pain CR perpendicular @ T7 |
| Oblique Ribs | CRITERIA: 45 degree oblique will shift spine away from anatomy of interest LPO/RAO = left axillary ribs RPO/LAO = right axillary ribs ribs 1-9 are seen on above diaphragm projections ribs 8-12 see on below diaphragm projections CR perpendicular @ T7 |
| with digital, if the mAs is too high your image will appear | brightness appropriate |
| with digital, if the IR is not exposed to enough radiation | image brightness will be appropriate quantum noise will be visible |
| increasing tube filtration will ___ | increase beam energy and decrease radiographic contrast |
| casts made of fiberglass require ______ in exposure factors | no change |
| to see soft tissues with DR, the standard exposure factors should be ______ | left the same because you can change window level to see tissues |
| Increasing SID will have what effect on your image? | will be sharper |
| what will happen to the contrast if the atomic number of the structure is increased? | contrast will increase due to increased absorption |
| When using the AEC, the RT must set the ____ | kVp |
| a higher kVp on an AEC exam results in ____ | shorter exposure time |
| When using AEC, what is the most critical aspect of performing the exam? | centering the anatomy of interest over the detector |
| what is a grid ratio? | the height of the lead strips inside the grid vs. the space between them |
| When you apply a grid during an exam what will happen to your contrast? | employing a grid will result in higher contrast in your image because less scatter is reaching the IR |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.