11947961
Descrição
FlashCards por Laura Gennaro , atualizado more than 1 year ago
|
|
Criado por Laura Gennaro
quase 7 anos atrás
|
|
| Questão | Responda |
| Superficial fungal infections | -Limited to mucocutaneous surfaces, hair, nails -Treated with topical or Oral systemic antifungals |
| Deep fungal infections | -Spread systemically, invade tissues, destroy vital organs -May be endemic to certain geographic areas or opportunistic in immunodeficient individuals -Typically treated with IV, oral antifungals (amphotericin B, azoles) |
| Candida species normally reside... Infections are generally localized to... | -in skin, the mouth, GI tract, & vagina -Mucocutaneous surfaces: >>Vulvovaginal area >>Oral cavity >>Diaper rash >>Esophagus |
| What are our "white" candida infections of the oral cavity | -Pseudomembranous candidiasis (thrush) -Chronic hyperplastic candidiasis |
| What are our "red" candida infections of the oral cavity | -Erythematous (atrophic) candidiasis -Denture stomatitis -Median rhomboid glossitis -Angular chelitis |
|
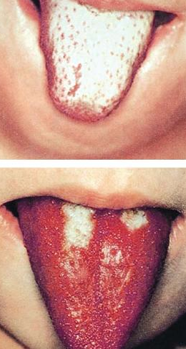
Pseudomembranous candidiasis
Image:
Image (binary/octet-stream)
|
-Curdy, white plaques/papules -characteristically wipeable and often reveals an erythematous base -Patients may complain of sensitivity or dysgeusia -Typically associated w/ some kind of (mild) immune suppression |
|
Chronic hyperplastic candidiasis
Image:
Image (binary/octet-stream)
|
-Solitary white plaque that cannot be rubbed off -Rarest clinical presentation of candidiasis -highly suspicious for leukoplakia; biopsy necessary for diagnosis |
|
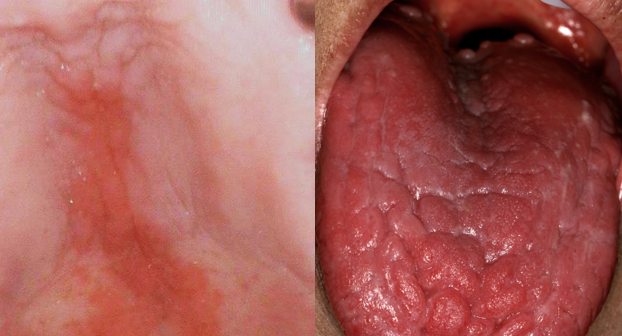
Erythematous (atrophic) candidiasis
Image:
Image (binary/octet-stream)
|
-erythematous, tongue dorsum atrophic when involved -Common presentation of candidiasis (together with pseudomembranous candidiasis) -Patient may complain of burning/sensitivity -May be seen following course of antibiotics or in context of dry mouth |
|
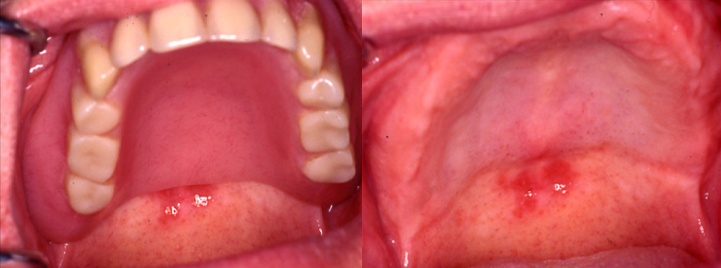
Denture stomatitis
Image:
Image (binary/octet-stream)
|
-erythematous candidiasis restricted to mucosa beneath a denture base -patient will admit to wearing their denture continuously |
| Differential diagnosis for denture stomatitis | (includes a few similarly-appearing but relatively rare etiologies) -Excessive pressure on mucosa (improper denture design) -Allergy to denture base -Inadequate curing of denture acrylic |
|
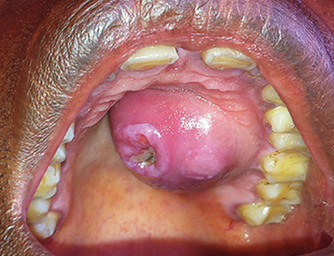
Median Rhomboid Glossitis
Image:
Image (binary/octet-stream)
|
-candidiasis involving the midline dorsum of the tongue -may present as a focal area of depapillation/atrophy and erythema or as area of nodularity -On occasion, a 'kissing' lesion may be present on the palatal mucosa |
| Differential diagnosis for median rhomboid glossitis | geographic tongue |
|
Angular cheilitis
Image:
Image (binary/octet-stream)
|
-erythema, maceration, scaling, fissuring of the corners of the mouth (usually bilateral, sometimes painful) -Caused by excessive moisture/maceration from saliva -Secondarily infected w/ Candida albicans; less commonly w/ Staph aureus -Especially common in denture-wearers and children -Should be distinguished from herpes labialis |
| Management of most forms of candidiasis | -Nystatin= mouth rinse -Clotrimazole troches= particularly good for treating median rhomboid glossitis -Fluconazole PO= systemic broad spectrum drug (contraindications/cautions include pregnancy, liver disease, renal disease, arrhythmia or arrhythmogenic medications) |
| Management of Denture stomatitis | -Apply miconazole cream onto denture base TID -Soak denture in solution overnight -Discontinue overnight wearing of denture |
| Management of angular cheilitis | -Clotrimazole ointment or cream -Improve denture fit/cleaning; use Vaseline as barrier cream |
| Chronic mucocutaneous candidiasis | -heterogenous group of syndromes characterized by noninvasive Candidal infections of the skin, nails, and mucous membranes -Caused by genetic defects of the immune system -Disease manifests within first few years of life |
| APECED Syndrome | -Mutations in AIRE (autoimmune regulator) -Autoimmune PolyEndocrinopathy -Candidiasis -Ectodermal Dystrophy |
| Aspergillosis | -Common causative agent of allergic fungal rhinosinusitis -Some patients are allergic to superficial infections of one or more fungi in the sinonasal tract -represents 5-10% of all chronic rhinosinusitis cases -Treated w/ surgical debridement, intranasal steroids |
| Superficial infection of aspergillosis may also present as... | Aspergilloma -represents a fungus ball comprised of aspergillus hyphae -Most common in pulmonary cavities, maxillary sinus -Symptoms are non-specific (resembles chronic sinusitis) -Treated by conservative removal |
| Deep Fungal infections | -usually endemic to certain geographic regions -Infections have acute, chronic, disseminated phases -Lungs usually the primary site of infection -Oral cavity, if involved, usually in context of chronic/disseminated disease (Oral cavity presentation non-specific and often suggestive of aggressive lesion or malignancy; biopsy required) |
| Deep Fungal infections: Histoplasmosis | Ohio & Mississippi river valleys -80-90% have been infected |
| Deep Fungal infections: Blastomycosis | Eastern half of US/Canada extending to the great lakes -9:1 male predilection |
| Deep Fungal infections: Paracoccidiomycosis | 'South American blastomycosis' -15:1 male predilection (female sex hormone seems to be protective) |
| Deep Fungal infections: Coccidiomycosis | Southwestern USA -(San Joaquin) Valley Fever -Rare hypersensitivity reaction |
|
Deep Fungal infections: Mucormycossi
Image:
Image (binary/octet-stream)
|
-Diabetic patients in ketoacidotic state particularly susceptible -Rhino-orbital-cerebral infection most common -Devastating, rapid disease progression requires immediate surgery & IV ampotericin B |
|
Deep Fungal infections: Cyptococcosis
Image:
Image (binary/octet-stream)
|
-Most commonly seen in setting of HIV/AIDS -Typically presents as cryptococcal meningitis |
| Cat Scratch Disease | -Self-limited regional lymphadenopathy -Caused by Bartonella henselae -Most common cause of regional lymphadenopathy in children -Results from scratch/bite of infected cat -80% of cases occur in 1st-2nd decade -5 day course of azithromycin preferred management |
| Clinical Features of Cat Scratch Disease | -Pustule/papule develops along initial scratch line -2-3 weeks later= Regional LAD, Fever/malaise -Lymph nodes tender -Overlying skin may be erythematous -Usually resolves over 1-4 months -Initial site of trauma often resolved by time of regional LAD |
|
Impetigo
Image:
Image (binary/octet-stream)
|
-Contagious superficial bacterial infection -Staph aureus is most common causative agent -Most frequently kids ages 2-5yr -May present as primary infection or normal skin or secondary impetiginization of previously damaged skin (abrasions, minor trauma, insect bites, eczema) |
|
Non-bullous Impetigo
Image:
Image (binary/octet-stream)
|
-Most common clinical presentation of impetigo -Erythematous papules and vesicles that form adherent crusts -Characteristic golden appearance -Regional lymphadenitis may occur |
|
Bullous Impetigo
Image:
Image (binary/octet-stream)
|
-Characterized by vesicles and flaccid bullae -Caused by specific strains of Staph aureus that produce exfoliative toxin A >>Targets desmoglein 1, resulting in loss of cell-cell adhesion |
| Treatment of Impetigo | Topical or oral therapy -Topical with limited skin involvement (remove scale w/ damp cloth; mupirocin, retapamulin for 5 days) -Oral when numerous lesions present (Dicloxacillin, cephalexin for 7 days) |
| Actinomycosis | -serious, chronic bacterial infection caused by Actinomyces -Many different clinical presentations >>Cervicofacial (55%) >>Abdominal (20%) >>Thoracic (15%) >>Others |
| Actinomycosis characteristic clinical features | -Chronicity & mass-like features w/ no respect for tissue boundaries -Sinus tract formation -Refractory/relapsing disease after short-course antibiotic therapy |
| Actinomycosis treatment | IV penicillin for 2-6 weeks followed by PO penicillin/amoxicillin for up to 6-12 months |
| Cervicofacial Actinomycosis ('lumpy jaw') | -most commonly presents as painless mass at angle of the jaw -firm, wooden consistency -slow, contiguous spread -LAD uncommon -Ill-defined radiolucency of jaw bones -Sinus tract formation with sulfur granules typically identified (represents bacterial colonies) |
| Actinomyces | -a part of the endogenous flora of mucous membranes (oral cavity, colon, vagina, bronchi) -disruption of mucosal barrier integral to pathogenicity of Actinomyces >>tooth extraction >>grossly carious tooth >>mandibular fracture |
| Syphilis | -Sexually transmitted disease caused by Treponema pallidum -Transplacental transmission occurs readily -Primary, Secondary, Tertiary, and Congenital |
| Primary Syphilis | -Chancre appears after 3-90 days at the site of sexual contact -characteristic ulceration -highly contagious (numerous treponemes present) -regional LAD present -Heals within 3-6 weeks even if untreated |
| Secondary Syphilis | -Occurs in 25-50% of untreated patients -Within 4-10 weeks of chancre -Diffuse/symmetric maculopapular skin rash involving the trunk, extremities, palms/soles -self-resolving but reappear -Generalized symptoms -Risk of transmission through intact skin low |
| Mucosal Lesions of secondary syphilis | -Mucous patches >>Contain numerous treponemes and are highly contagious -Condyloma lata |
| Tertiary Syphilis |
-Occurs in 25-40% of untreated patients
-Typically after a latent period of 1-30years
-Syphilitic involvement of heart/aorta, brain/nerves, eyes; death in some cases
-Nodular granulomatous lesions called gummas
Image:
Image (binary/octet-stream)
|
| Congenital Syphilis | -T. pallidum readily crosses the placenta, resulting in fetal infection -Risk is highest during untreated primary/secondary syphilis -Infection results in: >>Spontaneous abortion (40%) >>Premature birth >>Wide spectrum of clinical manifestations |
| Clinical Manifestations of Congenital Syphilis | -Skeletal syphilis is the most common manifestation of early disease -Hutchinson triad relatively specific presentation of late congenital syphilis: >>Hutchinson teeth (Hutchinson incisors, mulberry molars) >>Interstitial keratitis >>Sensorineural hearing loss |
| Diagnosis and Management of Syphilis | -Serologic testing of blood specimens >>Non-treponemal Ab tests >>Treponemal Ab tests -Tests have varying sensitivities during various stages and confirmatory testing necessary -Penicillin treatment of choice regardless of stage |
|
Scrofula
Image:
Image (binary/octet-stream)
|
-Oropharyngeal/cervical tuberculosis -Contracted by drinking milk contaminated w/ Mycobacterium bovis -Cervical lymphadenitis -Secondary ulceration, fistula, abscess formation -Same treatment as pulmonary TB -Lymph nodes may be calcified in severe/longstanding cases -Oral cavity lesions uncommon, generally occur in context of secondary/disseminated disease following primary pulmonary infection |
| Scarlet Fever |
-Represents delayed-type hypersensitivity reaction to S. pyogenes exotoxin
-Diffuse erythematous skin eruption
>>Clears within 1 week
>>Desquamates over 8 weeks
-Characteristic tongue changes over 5 days
-Generally occurs in association w/ strep pharyngitis
-Treatment directed towards underlying strep. pharyngitis
Image:
Image (binary/octet-stream)
|
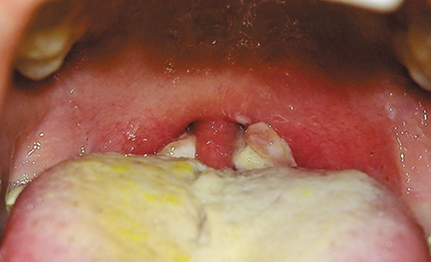
| Diphtheria |
-Serious infection caused by Corynebacterium diptheria
-Commonly presents as sore throat, low-grade fever, malaise, cervical LAD
-Gray, necrotic-appearing, firmly adherent pseudomembrane may develop over tonsils/pharynx
-Uncommon and readily preventable by DTP vaccine
Image:
Image (binary/octet-stream)
|
| Herpes Simplex Virus-1 (HSV-1) | -Typically affects oral, facial ocular areas -transmitted person/person via infected oral secretions during close contact -90% seropositivity worldwide by 4th decade -50-60% seropositivity in US (& declining) |
| Herpes Simplex Virus-2 (HSV-2) | -typically affects genital areas -transmitted sexually -15-20% seropositivity worldwide and in US -Greater in lower socioeconomic groups |
|
Primary Oral HSV Infection
Image:
Image (binary/octet-stream)
|
-Majority of infected children are asymptomatic -15-30% of children: herpetic gingivostomatitis -Self-limiting (10-20 days) ulcerative lesions of gingiva/entire mouth -May be accompanied by fever -Most symptomatic infections occur btwn 6months and 5yrs -Managed w/ supportive care (fluids, analgesics) >>Dehydration is most common complication >>Acyclovir may shorten disease course in some cases |
| Primary Oral HSV Auto-inoculations |
-Herpetic keratitis (major cause of blindness worldwide)
-Herpetic whitlow (resolves over 2-3weeks but may recur)
Image:
Image (binary/octet-stream)
|
| Latency | Persistence of viral genomes in cells that do not produce infectious virus -Orofacial HSV establishes latency in trigeminal ganglion |
| Recrudescence | -viral dissemination unaccompanied by tissue injury |
|
Herpes Labialis: clinical features
Image:
Image (binary/octet-stream)
|
Reactivation usually triggered by: -Stress -Immunodeficiency Self-limiting 5-10day course -prodromal symptoms 6-24hrs before visible lesions develop -Clusters of vesicles that rupture and crust within 2days |
| On average, how many recurrences of herpes labialis do patients experience annually | 2-10 |
| Herpes labialis vs. Angular Cheilitis | Herpes Labialis -rarely bilateral -typically painful -prodromal symptoms may be reported -self-limiting (heals within 5-7days) Angular Cheilitis -Exclusively on commissure of lips -frequently bilateral -typically painless -no prodromal symptoms -does not resolve on its own |
| Herpes labialis treatment | -Valacyclovir PO: 2g during prodrome; 2g 12hr later -Prophylactic valacyclovir for short-term use: 1g QD for duration of beach trips, ski vacations, etc. |
| Varicella-zoster virus (HHV-3) | -Historically greater than 95% seroprevalence in US -Varicella (chickenpox) affected almost everybody by age 20 -Self-limiting (1-2weeks) infection characterized by fever, malaise, generalized pruritic rash -younger onset= milder disease -Highly contagious |
| Recurrent VZV infection (herpes zoster; shingles) | -following primary infection (chickenpox), VZV establishes latency in sensory neurons >>dorsal root ganglia >>trigeminal ganglion (rare) -Viral reactivation with transport along sensory neurons to skin constitutes recurrent disease -estimated to affect 30% of the population |
| Shingles clinical appearance | -affected dermatome shows erythema, vesicle formation, ulceration -prodromal pain may precede for days/weeks -thoracic, lumbar dermatomes most commonly involved |
| Epstein-Barr virus (HHV-4) | -Approximately 90-95% seropositivity worldwide (majority of primary infections subclinical) -Cause of many diseases >>Infectious mononucleosis >>Lymphomas, nasopharyngeal carcinoma >>EBV mucocutaneous ulcer, hairy leukoplakia |
|
Infectious mononucleosis
Image:
Image (binary/octet-stream)
|
-acute illness due to EBV infections -Occurs mainly in adolescents, young adults -Characterized by fever, pharyngitis, fatigue, tender cervical LAD -Palatal petechiae may be present -managed w/ supportive therapy |
| Coxsackievirus | -Most infections asymptomatic/subclinical -Symptomatic infections usually affect infants & young children >>Hand, foot, and mouth disease >>Herpangina >>Acute lymphonodular pharyngitis (less common, overlapping features of HFMD/Herpangina) -Oral-fecal transmission |
| Hand, foot, & mouth disease | -Self-limiting disease (7-10 days) -Clinical diagnosis -Supportive care only -No/low-grade fever (< 101°F) -Erythema and small papuloulcerative lesions involving: >>Fingers >>Toes >>Oral cavity: typically anterior |
| Herpangina | -Self-limiting disease (7-10 days) -Clinical diagnosis -Supportive care only -High fever (> 102°F) -Erythema and small papuloulcerative lesions involving: >>Pharynx: less than 10 |
| Measles |
-caused by morbillivirus genus (uncommon w/ routine MMR vaccination)
-Highly contagious viral illness with 9-day course
>>Fever, malaise, cough, rhinitis
>>Erythematous (morbilliform) rash
>>Koplik spots on buccal mucosa (Represent foci or epithelial necrosis)
>>Complications in up to 40% of patients
-fatality rate as high as 25% in countries w/ low vaccine coverage
Image:
Image (binary/octet-stream)
|
| Mumps (epidemic parotitis) | -Caused by paramyxovirus genus -highly infectious and spread by respiratory droplets -most common viral cause of sialadenitis -Acute, self-limited viral syndrome >>approximately 2week duration >>sporadic outbreaks still occasionally occur in spite of routine MMR vaccination -Treatment symptomatic/palliative |
| Sialadenitis | infection of salivary glands |
| Clinical features of mumps | -low-grade fever, malaise, headache, myalgia -Parotitis in 95% of cases; bilateral in 90% -Lasts approx. 10 days -Increased serum amylase -Epididymoorchitis w/ testicular pain & swelling (40% of males; impaired fertility may result, sterility rare) -Oophoritis, pancreatitis -Aseptic meningitis |
|
Kaposi Sarcoma
Image:
Image (binary/octet-stream)
|
-vascular disorder/neoplasm resulting from HHV-8 infection -Most prevalent tumor among AIDS patients (incidence has decreased ~90% since introduction of ART) -60-70% of HIV/AIDS patients w/ KS have oral involvement -Oral cavity involvement in 2-5% of non-epidemic cases -Occurs in 4 distinct clinical settings |
| Classic KS | -indolent cutaneous lesions in elderly males of Eastern European/Mediterranean descent |
| African endemic KS | 3 major subtypes -Indolent cutaneous form (similar to classic type) -Locally aggressive cutaneous form -Aggressive form presenting in childhood (generalized LAD, with/without cutaneous lesions, rapidly fatal) |
| Iatrogenic KS | rare complication of immunosuppression |
| Epidemic/AIDS-associated KS | widespread mucocutaneous lesions in patients with AIDS -Strong predilection for homosexual men |
| Presentation of Kaposi Sarcoma | Presentation similar regardless of clinical setting: -Patch stage: early macules -Plaque stage: plaques -Tumor stage: progression to larger nodules |
| ART in HIV/AIDS | Anti-retroviral Therapy -should be administered early following infection as possible, regardless of CD4 count (associated w/ improved outcomes) -ART is a cocktail of: >>Nucleoside & non-nucleoside reverse transcriptase inhibitors >>protease inhibitors >>fusion inhibitors >>integrase inhibitors >>CCR5 inhibitors |
| HIV Infection | don't hate me but I really got lazy and I feel like we've been over this enough that I don't want to make flashcards for it |
| AIDS is defined by... | -CD4 T-cell count <200cells/uL >>Average time from HIV acquisition to CD4 T-cell count < 200 cells/μL: 8-10 years in untreated patient (normal CD4 count: 500-1500 cells/μL) -Presence of any AIDS-defining illness >>main contributors to morbidity/mortality prior to introduction of ART |
| Some of the more common AIDS-defining illnesses | -Pneumocystis jiroveci pneumonia -Esophageal candidiasis -Kaposi Sarcoma -Disseminated Mycobacterium avium infection |
| Oral & Maxillofacial lesions seen in HIV/AIDS | -Candidiasis (most common intraoral manifestation of HIV) -Hairy Leukoplakia (sign of advanced disease) -Kaposi sarcoma -Persistent generalized LAD -Necrotizing ulcerative gingivitis/periodontitis -Diffuse HPV lesions -HIV salivary gland disease -Increased cancer risk |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quer criar seus próprios Flashcards gratuitos com GoConqr? Saiba mais.