2530787
Descrição
FlashCards por Sameet Govan, atualizado more than 1 year ago
|
|
Criado por Sameet Govan
quase 10 anos atrás
|
|
| Questão | Responda |
| Most common type of headache | Tension headache |
| Intracranial pain sensitive structures | Venous sinuses, cortical veins, basal arteries, dura of anterior, middle and posterior fossae |
| extracranial pain sensitive structures | scalp vessels and muscles, orbital contents, mucous membranes of nasal and paranasal spaces, external and middle ear, teeth and gums |
| what is costen's syndrome | Tempromandibular joint dysfunction aching pain around the ear due to malalignment of one tempromandibular joint as consequence of dental loss with altered bite or involvement of the joint in RA requires dental treatment with realignment |
| what drug to avoid in migraine (analgesic) | opiates |
| webers and rinnes which tuning fork | 512khz |
| Webers interpretation | if sound lateralises then there is : an ipsilateral conductive hearing loss a contralateral sensorineural hearing loss |
| Rinne's interpretation | when nerve deafness is present then the note is audible at the external meatus, as air and bone conduction are reduced equally, so that the air conduction is better (as is normal) than bone conduction - this is termed Rinne-positive Rinne-negative occurs with a conductive hearing loss - no note is audible at the external meatus (i.e. bone conduction is better than air conduction) |
| which children with otitis media with effusion require immediate specialist referral | downs and cleft palate |
| menieres disease in a nutshell | paroxysm of up to 12 hours of rotational vertigo, hearing loss and tinnitus oftena feeling of fullness |
| how to assess for stroke in A&E | ROSIER scale. score over 0 is suggestive |
| stroke internal carotid artery occlusion | affected conscious level homonomous hemianopia of contralateral side contralateral hemiplegia contralateral hemosensory disturbance gaze palsy to opposite side partial horners occlusion of dominant hemisphere will result in global aphasia may get amaurosis fugax |
| anterior cerebral stroke | depends on site of occlusion and on anatomical variation Distal occlusion - weakness and cortical sensory loss in contralateral lower limb with associated incontinence, occasional contralateral grasp reflex Proximal occlusion - cerebral paraplegia (lower half of body), lower limb weakness, sensory loss, incontinence and presence of grasp, snout and plamomental reflexes bilateral frontal lobe infarction result in akinetic mutism |
| middel cerebral artery stroke | features depend on site and whether dominant or non-dominant affected occlusion at insula - contralateral hemiplegia, leg relative spared contralateraln hemiplegia and hemianaesthesia all cortical branches involved - aphasia (dominant) Non-dominant - neglect of contralateral limb and dressing difficulty parietal branch alone - wernickes dysphasia with no limb weakness deep branches - perforating vessels, of middle cerebral artery --> lacunar (discussed elsewhere) |
| vertebral artery occlusion | when low in neck - compensated by anastomosis only posterior inferior cerebellar solely dependent on this so may present as PICA syndrome - Vertigo, nausea and truncal ataxia are the most common presenting features. Signs of a lateral medullary syndrome |
| basillar artery occlusion | prodromal symptoms common - may have diplopia, visual field loss, intermittent memory disturbance and other brainstem symptoms complete basillar syndrome - impairment of consciousness (coma), bilateral motor and sensory dysfunction, cerebellar signs, cranial nerve signs indicvative of level of occlusion Top of basillar occlusion - lateral midbrain, thalamic and medial temporal lobe infarction abnormal movements (hemiballismus) are associated with visual loss, papillary abnormalities, gaze palsies, impaired conscious level and disturbances of behaviour Paramedian perforating vessel occlusion gives rise to locked in syndrome and lacunar infarction |
| posterior cerebral artery occlusion | proximnal occlusion - III nerve palsy and contralateral hemiplegia - Weber syndrome, Thalamic structures - chorea (spasmodic movements (said vituses dance)) occlusion of cortical vessels - different picture with visual feild loss (homonomous hemianopia) and sparing of macular region, which is supplied by the middle cerebral if the above happens in the dominant hemisphere then may have problems naming colours and objects |
| cerebellar arteries | superior, anterior and posterior lesions in their territory would also produce brainstem symptoms and signs localising to superior pontine, inferior pontine and medullary levels respectively |
| superior cerebellar artery syndrome | Cerebellum - distubed gait, limp ataxia Brain stem - inspilateral horners, contralateral sensory loss to pain and temp |
| anterior inferior cerebellar artery syndrome | cerebellum - ipsilateral limb ataxia Brtain stem - inspilateral: horners, sensory loss to pain and temp, facial weakness, paralysis of lateral gaze contralateral sensory loss - pain and tempo of limbs of trunk |
| posterior inferior cerebellar artery syndrome | AKA lateral medullar syndrome Cerebellum - dysarthria, ipsilateral limb ataxia and nystagmus Brain stem - ipsilateral: Horner's, sensory loss to pain/temp of face, pharyngeal and laryngeal paralysis; and contralateral sensory loss to pain and temp of limbs and trunk |
| basilar artery paramedian branch occlusion | Midbrain level - complete or partial III nerve palsy, damage to red nucleus (outflow from opposite cerebellar hemisphere) will also produce contralateral tremor referred to as Benedickt's syndrome Pontine level - VI and VII nerve palsy (ipsilateral) and contralateral sensory loss to light touch, proprioception, when the lesion is more basal When the nerve palsies are accompanied by contralateral hemiplegia - Millard-Gubler syndrome At medullar level - locked in syndrome, paralysed and unable to talk, some facial and eye movements are preserved. spinothalamiuc sensation retained, but involvement of the medial meniscus produces discriminatory sensation in the limb |
| where to cortical infarcts occur | 80% in periventricular white matter and basal ganglia, rest in cerebellum and brain stem 17% of all thromboembolic strokes |
| lacurnar stroke syndromes | Pure motor Pure sensory Dysarthria/clumsy hand ataxic hemiparesis severe dysarthria with facial weakness |
| important things to exclude before TIA | Migraine, partial seizure, hypoglycaemia, syncope, hyperventilation |
| risk assessment in patient with TIA but no neurological symptoms | ABCD2 score score of (any, low and high risk) or more then aspirin or clopidogrel each as 300mg loading dose then 75mg thereafter and a statin (40mg Simvastatin) According to RCP if giving aspirin then should give with dypiridamole Guidelines may change to aspirin and clipidogrel in future |
| who can be high risk of stroke even if ABCD2 score is less than 4 | Crescendo TIA (two or more TIAs in a week), AF, or those on anticoagulation |
| ABCD2 low risk of stroke score <=3 | same as high risk but just need to be seen in a week vs 24hrs |
| who should have carotid imaging | all with suspected non-disabling stroke or TIA who after specialist assessment are considered as candidates for carotid endarterectomy image in 1 week also those with symptomatic carotid stenosis, suregy less than 2 weeks in this group |
| primary and secondary prevention of stroke` | JBS2, Qrisk2 and ETHRISK |
| in diabetes where might hard exudates be found | around the macula in a star formation or around clumps and rings surrounding microaneurysms |
| primary open angle glaucoma | commonest form, reduced outflow of aqueous humor |
| treatment of primary open angle glaucoma | bet blocker e.g. timolol (reduces aqeuous production), prostaglandin analogues e.g. lantaprost (increases aqeous outflow), carbonic anhydrase inhibitors (acetozolamide), reduces aqeuos production |
| normal pressure glaucoma | glaucomatous changes but normal pressure Can reduce IOP can trabeculectomy |
| acute angle colsure glaucoma | emergency occlusion of trabecular meshwork by the peripheral iris - iridotrabecular contact, obstructing aqueous flow suddeen rise in pressure >50mmHg due to reduced aqeuous drainage of ageing lens pushing iris forward Most at risk are hypermetropes and women sudden onset red painful eye with blurred vision. eye is injected, tender and feels hard Pharm treatment - can use acetozolamide, beta-blockers, PG analogues, pilocarpine to constrict the eye and apraclonidine Analgesia and antiemetics |
| symptoms of macula dysfunction | Metamorphobsia - distorted vision Micropsia and macropsia - smaller or larger vision |
| discharge and type of conjunctivitis | Mucopurulent - bacteria Watery - viral, chalamydial allergic - stringy |
| bitemporal hemianopia and location of pathology based on which section lost first | top lost first - compression from below Bottom lost first - compression from the top |
| Simple partial vs complex partial seizure | Simple no loss of consciousness Complex - loss of consciousness |
| Tools for assessment of disability or needs in elderly people | Barthel's index Functional independence measure and functional assessment measure (FIM-FAM) Northwick park dependency scale Camberwell assessment of need in the elderly |
| initial dopamine treatment | Dopamine agonist (non-ergot) such as ropinerole, pramipexole, rotigotine Or Levodopa and a comt inhibitor such as Entacapone or Tolcapone which reduces the metabolism of levodopa |
| other parkinsons treatment other than dopamine agonist and levodopa | selegiline and resagiline - MAO type B inhibitors which reduce breakdown of DOPA Amatadine - useful for reducing dyskinesias late in disease Apomorphine injection or continuous infusion - strong dopamine agonist Domperidome for nausea antimuscarinics such as orphenadrine, procyclidine, trihexyphenidyl hydrochloride |
| Folstein MMSE score to suspect cognitive impairment | <24 |
| AMTS score which suggests dementia | <6 |
| who is at risk of falls | all over 65 patients aged 50-64 who are judged to be at higher risk don't use falls risk assessment tools |
| fracture prevention groups | Prevent falls HRT Bisphosphonates Manage risk factors for osteoporosis - vit D and calcium (prescribed for those in nursing home) |
| two types of pathology in peripheral neuropathy | Axonal (often metabolic) Demyelinating (often autoimmune) do neurophysiological tests to distinguish between them |
| commonest cause of acute symmetrical peripheral neuropathy | guillain barre |
| commonest cause of acute multiple mononeuroapthy | vasculitis - emergency |
| typical foot shape in charcot marie foot disease | High arched and hammer toes |
| charcot marie tooth disease | inherited neurological disorder weakness of the foot and lower leg muscles, which may result in foot drop and a high-stepped gait with frequent tripping or falls Foot deformities, such as high arches and hammertoes Lower legs may take on inverted champagne bottle appearance Later in the disease, weakness and muscle atrophy may occur in the hands, resulting in difficulty with carrying out fine motor skills Onset of symptoms is most often in adolescence or early adulthood, but some individuals develop symptoms in mid-adulthood. The severity of symptoms varies greatly among individuals and even among family members with the disease. |
| Importance of reflexes in Proximal muscle weakness | diminished or absent then polyneuropathy Present - myopathy |
| Limb weakness with variable intensity | neuromuscular junction pathology |
| myotonic dystrophy | failure of muscle relaxation after contraction. hit hand with tendon hammer and watch dimple persist. hard to let go of something facies distal |
| polymyositis and dermatomyositis | systemic symptoms first, lassitude, then muscle weakness. Oedema of skin and subcut tissue common in periorbital region dermatomyositis has violet discoloured skin rash often at sun exposed sites and can ulcerate proximal weakness to both with head lollingforward |
| secondary causes of proximal weakness | Acromegaly Hyperparathyroidism and osteomalacia Hyper and hypoadrenalism hyperthyroidism hypothyroidism |
| Things that do not happen in motor neuron disease | sensory signs do not occur Bladder is never involved Ocular muscles are never affected |
| only approved drug for motor neuron disease | Riluzole - has antiglutamate properties |
| summary of eyelid problems | Eyelid problems commonly encountered include: blepharitis: inflammation of the eyelid margins typically leading to a red eye stye: infection of the glands of the eyelids chalazion (Meibomian cyst)-more rounded and no yellow head entropion: in-turning of the eyelids ectropion: out-turning of the eyelids Stye Different types of stye are recognised: external (hordeolum externum): infection (usually staphylococcal) of the glands of Zeis (sebum producing) or glands of Moll (sweat glands). internal (hordeolum internum): infection of the Meibomian glands. May leave a residual chalazion (Meibomian cyst) management includes hot compresses and analgesia. CKS only recommend topical antibiotics if there is an associated conjunctivitis A chalazion (Meibomian cyst) is a retention cyst of the Meibomian gland. It presents as a firm painless lump in the eyelid. The majority of cases resolve spontaneously but some require surgical drainage |
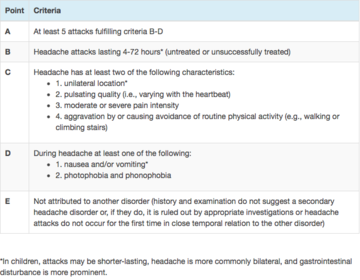
| Migraine classification according to international headache classification | |
| Migraine symptoms requiring secondary referral | motor weakness double vision visual symptoms affecting only one eye poor balance decreased level of consciousness. |
| Otitis externa management | mild cases (mild discomfort and/or pruritus; no deafness or discharge), consider prescribing topical acetic acid 2% spray. eatures of more severe inflammation are present, advise 7 days of a topical antibiotic with or without a topical steroid. The NICE Clinical Knowledge summary suggests that inflammation is more likely to be severe if there is: a red, oedematous ear canal which is narrowed and obscured by debris conductive hearing loss discharge regional lymphadenopathy cellulitis spreading beyond the ear fever |
| Acute management of stroke | ABCDE blood glucose, hydration, oxygen saturation and temperature should be maintained within normal limits blood pressure should not be lowered in the acute phase unless there are complications e.g. Hypertensive encephalopathy* aspirin 300mg orally or rectally should be given as soon as possible if a haemorrhagic stroke has been excluded with regards to atrial fibrillation, the RCP state: 'anticoagulants should not be started until brain imaging has excluded haemorrhage, and usually not until 14 days have passed from the onset of an ischaemic stroke' if the cholesterol is > 3.5 mmol/l patients should be commenced on a statin. Many physicians will delay treatment until after at least 48 hours due to the risk of haemorrhage transformation Thrombolysis - alteplase recommended. within 4.5 hours of symptom onset and where haemorrhage definitely excluded. (look up absolute and relative contraindications) Anticoagulation - clopidogrel first line over aspirin (75mg) and dypiridamole combination when to carotid endarterectomy: see next card |
| when to consider carotid endarterectomy in stroke pt | recommend if patient has suffered stroke or TIA in the carotid territory and are not severely disabled should only be considered if carotid stenosis > 70% according ECST** criteria or > 50% according to NASCET*** criteria |
| Two broad classifications of seizures | General Focal (AKA partial) |
| Types of general seizure | Absence, myoclonic, tonic, tonic-clonic and atonic discharge arises in both hemispheres consciousness lost immediately |
| types of focal seizure | Frontal - motor phenomena temporal - auditory or sneosry phenomena occipital - positive or negative visual phenomena parietal - contralateral altered sensation (dysaesthesia) Arise from one part of one hemisphere simple (no disturbance of consciousness or awareness) complex (consciousness is disturbed) |
| what is west syndrome | age 4-6 months seizure - violent flexor spasm of head, trunk and limbs followed by extension of arms (salaam spasms). flexor lasts 1-2s, often multiple bursts of 20-30 spasms. may occur many times a day. social interaction often deteriorates. |
| what is lennox-gastaut syndrome | multiple seizure types, mostly drop attacks (astatic seizures), tonic seizures and atypical absences. also neurodevelopmental arrest or regression and behaviour disorder. poor prognosis. |
| Childhood absence epilepsy | stare momentarily and stop moving. may have twitch of eye or hand. lasts only few seconds. child has no recall developmentally normal but can interfere with schooling. Accounts for only 2% of childhood epilepsy Can induce episodes by hyperventilation Good prognosis |
| what is benign epilepsy with centrotemporal spikes | 4-10 years old tonic clonic seizures in sleep, or simple focal seizures with awareness of abnormal feelings in the tongue and distortion of the face (supplied by the rolandic area of the brain) Almost all remit in adolescence |
| What is Early-onset benign childhood occipital epilepsy (Panayiotopoulos type) | 1-14 years younger children - periods of unresponsiveness, eye deviation, vomiting and autonomic features Older children - headache and visual disturbance including distortion of images and hallucinations. |
| what is juvenile myoclonic epilepsy | Adolescence to adulthood Myoclonic seizures, but generalised tonic-clonic seizures and absences may occur, mostly shortly after waking Typical history is throwing drinks or cornflakes about in the morning. Genetic linkage Remission unlikely but good response to life-long meds. |
| How to diagnose epilepsy, when to image and when to treat | Diagnose - history, video evidence, EEG Image - when neurological signs between seizures, or if seizures are focal, in order to identify a tumour, vascular lesion, or area of sclerosis which could be treatable Usually only treat with antiepileptic after second seizure. |
| Which drug not to use in women of child bearing age with epilepsy | sodium valproate. |
| epilepsy drugs real simple according to NICE | sodium valproate can be used first line for virtually all epilepsy except - status epilepticus and infantile spasms Second line or women Lamotrigine can be used in all except - myoclonic (use levitiracetam), all the ones that soidum valproate can't be used in, Dravet syndrome (use clobazam or stiripentol) |
| acute and prophylactic management of migraine | Migraine acute: triptan + NSAID or triptan + paracetamol prophylaxis: topiramate or propranolol |
| How does baclofen work and what is it used for | activates GABA receptors, many [GABAb] receptors are located on the presynaptic nerve terminal and activation results in reduced neurotransmitter release. good for controlling muscular spasms that occur in diseases such as MS |
| name the 3 acetylcholinesterase inhibitors used in Alzheimer's disease | Donepezil, galantamine, rivastigmine |
| what is the following Cutaneous features depigmented 'ash-leaf' spots which fluoresce under UV light roughened patches of skin over lumbar spine (Shagreen patches) adenoma sebaceum (angiofibromas): butterfly distribution over nose fibromata beneath nails (subungual fibromata) café-au-lait spots* may be seen Neurological features developmental delay epilepsy (infantile spasms or partial) intellectual impairment Also retinal hamartomas: dense white areas on retina (phakomata) rhabdomyomas of the heart gliomatous changes can occur in the brain lesions polycystic kidneys, renal angiomyolipomata lymphangioleiomyomatosis: multiple lung cysts | Tuberous sclerosis |
| Pre auricular lymph nodes in conjunctivitis is most likely to be what? | Bacterial or viral conjunctivitis may be associated with a purulent discharge and bilateral symptoms where as preauricular lymph nodes are only a feature of viral or Chlamydial conjunctivitis |
| MOA of sodium valproate and lamotrigine | use dependent block of neuronal Na+ channels Valproate also reduces the calcium current in calcium channels and dampen the thalmococortical oscillations that are critical in generation of absence seizures |
| What is ethosuximide good for | absence seizure and myoclonic seizures |
| what is carbidopa and benserazide | extracerebral decarboxylase inhibitors used to reduce extra cerebral metabolism of antiparkinsonian drugs |
| which drug can be given to reduce peripheral side effects of dopaminergic drugs | Domperidone - dopamine antagonist that does not penetrate the blood brain barrier. |
| what does entacapone do and how does it work | inhibits catechol-O-methyltransferase (COMT) and prevents the peripheral conversion of levodopa to 3-methoxydopa. increases the plasma halflife of levodopa and increases its action |
| side effects od dopaminergic drugs | nausea, psychiatric symptoms, postural hypotension, daytime somnolence, impulse control disorders, e.g. gambling and hypersexuality |
| alternative starting therapy option in parkinson's | dopamine agonist (non-ergot) such as ropinirole and rotigotine and a MAOb inhibitor such as selegiline and rasagiline |
| drug used to manage 'off' periods in parkinsons | apomorphine |
| How to MAOb inihibitors work | inhibit MAOb in the brain and can delay the need for levodopa Also can be used as an initial therapy with a dopamine agonist such as ropinorole |
| When to start parkinsons disease treatment | delay treatment until the onset of disabling symptoms and then to introduce a dopamine receptor agonist. If the patient is elderly, levodopa is sometimes used as an initial treatment. |
| medication to prescribe in SAH | Calcium-channel blockers should be started on admission for vasospasm prophylaxis. Calcium-channel blockers reduce risk of poor outcome and secondary ischaemia after aneurysmal SAH. Primary options nimodipine: 60 mg orally every 4 hours for 21 days Also - stool softener, anti tussative, analgesia, coagulopathy correction, sodium correction, |
| Causes of optic neuritis and its features | Causes multiple sclerosis diabetes syphilis Features unilateral decrease in visual acuity over hours or days poor discrimination of colours, 'red desaturation' pain worse on eye movement relative afferent pupillary defect central scotoma Management high-dose steroids recovery usually takes 4-6 weeks Prognosis MRI: if > 3 white-matter lesions, 5-year risk of developing multiple sclerosis is c. 50% |
| Two broad classifications of diabetic retinopathy and the features | Proliferative and non-proliferative (NPDR) Mild NPDR 1 or more microaneurysm Moderate NPDR microaneurysms blot haemorrhages hard exudates cotton wool spots, venous beading/looping and intraretinal microvascular abnormalities (IRMA) less severe than in severe NPDR Severe NPDR blot haemorrhages and microaneurysms in 4 quadrants venous beading in at least 2 quadrants IRMA in at least 1 quadrant Proliferative retinopathy retinal neovascularisation - may lead to vitrous haemorrhage fibrous tissue forming anterior to retinal disc more common in Type I DM, 50% blind in 5 years Maculopathy based on location rather than severity, anything is potentially serious hard exudates and other 'background' changes on macula check visual acuity more common in Type II DM |
{kind=link}
Quer criar seus próprios Flashcards gratuitos com GoConqr? Saiba mais.