2921915
Descrição
FlashCards por Sameet Govan, atualizado more than 1 year ago
|
|
Criado por Sameet Govan
mais de 9 anos atrás
|
|
| Questão | Responda |
| What is pharmacodynamics | what drug does to body |
| what is pharmacokinetics | the way the body affects the drug with time (absorption, distribution, metabolism and excretion) |
| strength of binding of drug to receptor is called what? | affinity |
| selectivity of drug to bind to receptor is called what? | specificity |
| which drug abolishes anticoagulant effect of heparin | protamine |
| what time of decay to most drugs have from the blood stream | exponential (a constant fraction eliminated) |
| how are most drugs eliminated | renally |
| How to increase rate of aspirin renal excretion | bicarbonate makes the urine alkaline, making the aspirin ionised and less lipid soluble |
| Liver phase I reaction | biotransformation of a drug to a more polar metabolite. most often by oxidations but also reductions and hydrolysis |
| liver phase II reaction | drug or phase I metabolites made more polar to be rapidly excreted from the kidneys and more hydrophilic by conjugation with endogenous liver compounds |
| drugs that are enzyme inducers | Phenobarbital, carbamazepine, ethanol (chronic), rifampicin, tobacco smoke, polycyclic aromatic hydrocarbons |
| Cimetidine inhibits the metabolism of which drugs erythromycin inhibits the metabolism of which drugs | cimetidine - phenytoin, warfarin, theophylline erythromycin - theophylline, warfarin, carbamazepine and digoxin |
| General MOA or local anaesthetics and some examples | weak bases --> penetrate nerve in lipophilic form --> some become ionised an block the Na channels --> prevents generation of action potentials Lidocaine, bupivicaine |
| Unwanted effects of local anaesthetics | synthethic agents - sedation, lightheaded ness, anxiety restlessness, higher doses - twitching and visual disturbances, severe toxicity - convulsions, coma, resp and cardiac depression CV - all except cocaine cause vasodilation, cocaine vasoconstricts |
| examples of acetylcholiesterases and what they are used to treat | neostigmine, pyridostigmine |
| what to use edrophonium for | very short acting, diagnose myasthenia gravis |
| neuromuscular blocking drugs | muscle relaxant competitive antagonists - reduce endplate depolarisation (pancuronium, vercuronium, atracurium, cisatracurium, rocuronium) Depolarising blockers - trigger opening of ion channels - suxamethonium Some presynaptic agents prevent release of Ach - botulinum toxin (aminoclycosides such as gentamicin may cause neuromuscular blockade by inhibiting calcium reflux) |
| neuromuscular blocking drug to use in severe renal or liver failure | atracurium |
| what are cholinomimetics | drugs that mimic the effects of acetylcholine 2 types. ones that act at Ach receptors and some that inhibits acetylcholinesterase to allow Ach to accumulate |
| Alpha 2 blocker examples and MOA | Clonidine and methyldopa - an alpha 2 agonist - centrally acting hypotensive |
| What does phenylephrine do? | alpha 1 agonist - decongestant and mydriatic |
| alpha 1 blocker name and use | Prazosin hypertension, can cause reflex tachycardia to a degree |
| What to MAO and COMT do | catabolise catacholamines (think parkinson also) |
| what does activation of alpha adrenoreceptors lead to | vasoconstriction or glandular secretion |
| What does activation of alpha 2 adrenoreceptors do | diminishes further transmitter release |
| How to indirect sympathomimetics work and examples | resemble norepinephrine so are taken up and displace vesicular norepinephrine into cytoplasm and then out of nerve terminal |
| beta blockers | more lipid soluble drugs more likely to enter brain and cause bad dreams |
| cardioselective beta blockers and asthma? | No! can cause bronchospasm still |
| how to reduce pressure in glaucoma | Increase aqueous outflow - prostaglandin analogue (latanoprost, travoprost) reduce aqueous formation with a beta blocker - timolol (can be absorbed and cause systemic effects) In closed angle if severe increase in pressure then need to rapidly reduce and can use pilocarpine eye drops, IV acetazolamide and IV hypertonic mannitol to remove water |
| which drug classes cause mydriasis | Muscarinic antagonists (atropine like drugs, cyclopentolate and tropicamide) and alpha adrenoreceptor agonists (phenylephrine) warning may precipitate acute closed angle glaucoma. |
| Drugs to cause miosis | Muscarinic agonists (pilocarpine) and alpha adrenoreceptor antagonists |
| Corticosteroid effect on the eye (bad) | cataracts |
| Recommended safe dose of lidocaine 1% and bupivicaine 0.25% | lido - 3mg/kg, bupiv - 2mg/kg |
| Max single dose of lidocaine 1% and bupivicaine 0.25% | lido - 200, bupiv - 150mg |
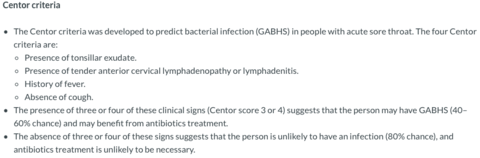
| Centor criteria | |
| Mecahnisms of drug resistance | Intrinsic - Inactivation of drug by enzymes, modified drug target, modified cell wall protein, activation of drug efflux pumps Evolution Acquired |
| drug resistant organisms of concern in the UK | Glycopeptide resistant enterococci (GRE), MRSA, Extended spectrum beta-lactamase (ESBLs)/carbapenemase produces CDiff resistant Candida sp |
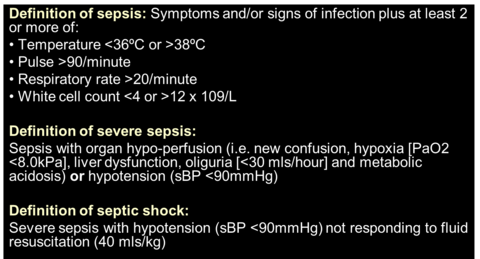
| Definition of sepsis severe sepsis septicv shock | |
| What is sepsis 6 | Oxygen IV fluid resuscitation Blood culturtes Antibiotics within 1 hour serum lactate Monitor urine output Anyone with sepsis should be admitted, oxygen mandatory only in severe and/or shock, IV fluids mandatory only in severe and/or shock |
| How is MRSA and most antibiotic resistance transmitted | usually person to person |
| Methiclillin resistance equates to which antibiotic | Flucloxacillin Practice point: penicillins, cephalosporins, carbapenems, monobactams (i.e. beta-lactams) are not effective in MRSA infections |
| what would you prescribe in methicillin resistance | glycopeptide such as vancomycin or teicoplanin |
| What can we do to prevent infections with resistant organisms | appropriate antibiotic prescribing, infection control practice, organisational culture/ethod, modify patient risk factors |
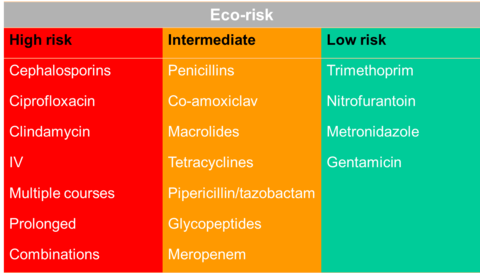
| ECO risk of drugs, high, intermediate, low | |
| Phenytoin precipitates in dextrose solutions Amphotericin precipitates in saline Gentamicin is physically/chemically incompatible with most beta-lactams these are examples of what type of drug interaction | Ex-vivo |
| sucrulfate, some milk products, antacids and oral iron preparations block absorption of what | Quinolones, tetracycline and azithromycin |
| Omeprazole, lansoprazole andH2 antagonists reduce absorption of what? | ketoconazole |
| Colestyramine binds which drugs | Raloxifene thyroid hormone digoxin |
| Cytochrome p450 3A4 responsible for metabolism of: | Most calcium channel blockers Most benzodiazepines Most HIV protease inhibitors Most HMG-CoA-reductase inhibitors Cyclosporine Most non-sedating antihistamines Present in GI tract and liver |
| inhibitors and inducers of CYP450 3A4 | Inhibitors Ketoconazole Fluconazole Cimetidine Clarithromycin Erythromycin Grapefruit juice (reduction in midazolam and simvastatin) Inducers Carbamazepine Rifampicin Rifabutin Ritonavir St. John’s wort |
| CYP2D6 metabolism of what and inhibited by what | metabolism of - codeine, many beta blockers, many tricyclic antidepressants inhibiterd by - fluoxetine, haloperidol, paroxetine |
| Cytochrome p450 2c9 | Primary metabolism of: Most NSAIDs (including COX-2s) S-warfarin (the active form) Phenytoin Inhibited by:Fluconazole |
| cyp 2c19 | Primary metabolism of: Diazepam Phenytoin Omeprazole Clopidogrel Inhibited by: Omeprazole Isoniazid Ketoconazole |
| Cyp1A2 | Catalyzes primary metabolism of: -Theophylline -Imipramine -Propranolol -Clozapine Inhibited by: -Many fluoroquinolone antibiotics -Fluvoxamine -Cimetidine Induced by smoking tobacco |
| examples of drug food interactions | Tetracycline and milk products Warfarin and vitamin K-containing foods, spinach, soya Grapefruit juice Bisphosphonates and food |
| grapefruit and statins | Lovastatin, atro and simvas - all increased bioavailability. Does not seem to have much effect on pravastatin and fluvastatin |
| St Johns wort | P450 3A inducer - reduce cocn of indinavir, ciclosporin, digoxin |
| Drug interactions with anti-retrovirals | Oral contraceptives (may require second method) Methadone Erectile dysfunction agents Herbs - St. John’s wort Lipid-lowering agents Anti-mycobacterials, especially rifampicin Psychotropics – midazolam, triazolam Ergot Alkaloids Antihistamines – astemizole Anticonvulsants |
| what does cooling blood samples do to potassium levels | Increases it slightly |
| Hypokalaemic, hypernatraemia | Cushings |
| cause of coma in severe type 2 diabetes | Hyperosmolar, non-ketotic (HONK)hyperglycaemia |
| tumour markers | PSA - prostate cancer Alpha-fetoprotein (AFP) - numerous cancers Carcinoembryonic antigen (CEA) - GI tract cancers CA19-9 - GI tract and pancreatic cancers CA-125 - ovarian cancers CA15-3 - breast cancers Paraprotein – myeloma Human chorionic gonadotrophin (hCG) - choriocarcinomas |
| some random points to remember | . Relationship between K+ and Mg+ levels… if you can’t correct hypokalaemia check the Magnesium levels ! 2. If you see the combination of Hyponatraemia, Hyperkalaemia and Hypoglycaemia on biochem lab results, don’t think about correcting each individually… MUST think of Addisonian Crisis in the acutely ill patient ! 3. Do not correct chronic hyponatraemia too rapidly. If you see hyponatraemia do not assume it acute. But check previous Na levels in notes 4. Hyperkalaemia and hypokalaemia can kill ! 5. When prescribing regular maintenance fluids for your patient…. Always check U&E's especially K+, Glucose and Creatinine. You can overload an elderly patient with poor renal function with just a litre of normal saline given too fast. |
| Type A (augmented) drug reaction | exaggerated reponse to pharmacological action Warfarin --> bleeding Beta blocker --> brady cardia Usually dose dependent High incidence, low mortality Secondary effects - can rationalise from pharmacology - beta blocker and bronchospasm |
| Type B (bizzare) drug reaction | abnormal effect low incidence, high mortality unpredictable Often necessitates withdrawal of drug Chloramphenical and aplastic anaemia |
| Other drug reactions Type C (Chronic treatment effects) osteoporosis with steroids Type D (Delayed effects) drug induced cancers Type E (End of treatment effects) withdrawal syndromes | Type C (Chronic treatment effects) osteoporosis with steroids Type D (Delayed effects) drug induced cancers Type E (End of treatment effects) withdrawal syndromes |
| other type A drug reactions | diarrhoea with antibiotics hepatic failure with paracetamol drug interactions - theophylline and clarithromycin, metabolism inhibited so increased toxicity |
| Mechanisms of type B idiosyncratic drug reactions | Abnormal biological system - primaquine induced haemolysis in G6PD deficiency (sex linked inherited defect), common in black americans, deficiency in reduced glutathione Abnormalities in drug metabolism - isoniazid and peripheral neuropathy (slow acetylators) Immunological - penicillin induce analphylaxis and steven's jhonson syndrome |
| Hx of anaphylaxis, urticaria or rash immediately after penicillin | DO NOT Rx a penicillin, cephalosporin or beta lactam antibiotic |
| penicillin allergy, do not use any of the following | Tazocin Co-amoxiclav Imipenem Meropenem |
| don't use flucloxacillin in which type of disorder | hepatic |
| cyclophosphamide class and specific side effects | Haemorrhagic cystitis - minimised by administration of Mesna, neutralises toxicity of drug hepatotoxic |
| Methotrexate class and specific side effects | Antimetabolite (folate) Specific side effects - mucositis, inflammation of the throat and mouth myelosuppression renal failure hepatotoxicity |
| Docorubicin class and specific side effects | Topoisomerase II inhibitor analogue Mucositis Cardiotoxic |
| 5-FU class and specific side effects | Antimetabolite (pyrimidine) Specific side effects - stomatitis, palmar-plantar erythrodysesthesia sydrome Rash and dry skin, photosensitive |
| Side effects and common drugs Nausea and vom alopecia hyperuricaemia neurtropaenia | nausea and vom-cisplatin Alopecia - frequencies of chemotherapy-induced hair loss differing across the four major drug classes: >80% for antimicrotubule agents (e.g., paclitaxel), 60%-100% for topoisomerase inhibitors (e.g., doxorubicin), >60% for alkylators (e.g., cyclophosphamide), and 10%-50% for antimetabolites (e.g., 5-fluorouracil plus leucovorin) hyperuricaemia cause by tumour lysis syndrome - allopurinol can be given to help prevent against gout |
| often drug causes conditions anaphylaxis stevens-johnson syndrome blood dyscrasias | Anaphylaxis antibiotics, iron dextran injection Stevens-Johnson Syndrome associated with carbamazepine, antibiotics Blood dyscrasias neutropenia with methotrexate thrombocytopenia with heparin |
| highly protein bound drugs and factors which can affect that | > 95% bound Thyroxine Warfarin Diazepam Frusemide Heparin Aspirin Amitriptylline > 90% bound Glibenclamide Phenytoin Propranolol Sodium Valproate Low plasma albumin levels (<20-25g/L) e.g. liver d., kidney d., late pregnancy Displacement e.g. aspirin, valproate, sulphonamides Saturation of plasma protein binding within therapeutic range e.g. phenytoin |
| Liver disease leads to hiugh concentrations of what | tamazepam, morphine, nifedipine, omeprazole, ethanol |
| things that interfere with the pill | extensive enterohepatic recirculation, therefore bile acid sequestrants and broad spectrum antibiotics |
| drugs with high renal excretion | Opiods Aminoglycosides Digoxin Lithium |
| lithium adverse effects | thyroid disorders diabetes insipidus cognitive and memory impairment Sodium depletion, warning with diuretics |
| helicobacter eradication triple therapy | PPI Plus 2 of the following - clarithromycin, metronidazole, amoxicillin All twice daily for 7 days |
| drugs in UC and Chron's | UC - 5ASA, salicylate (mesalasine), additional things are steroids, ciclosporin, tacrolimus, infliximab immunosupprssants for Chron's - Azathioprine and 6 mercaptopurine (they reduce T lymphocytes), side effects - low WBCs, nausea, vomiting, pancreatitis Chron's can also use anti TNFs - infliximab and adalimumab. Can also use steroids |
| 5ht4 receptor agonist for chronic constipation | prucalopride |
| GCC agonist | Linaclotide |
| side effects of beta blockers | depression fatigue sexual |
| angina treatments | Slow heart rate beta blockers rate limiting calcium antagonists (verapamil, diltiazem) If inhibition - ivabradine |
| angina vasodilators | Dihydropyridine calcium antagonists (e.g. amlodipine and nifedipine) Nicorandil |
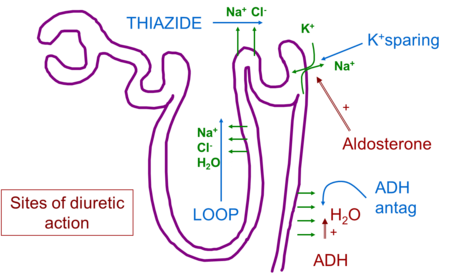
| site of action of diuretics | |
| Loop diuretics | e.g. frusemide Block Na+/K+/2Cl- co-transporter in thick ascending limb of loop of Henlé Work from the lumen of the tubule “High ceiling” Hyponatraemia, hypokalaemia, hyperuricaemia |
| Thiazide diuretics | e.g. bendroflumethiazide, metolazone Block Na+/Cl- co-transporter in DCT “Low ceiling” Loss of Na+, K+, Mg++ Increase in urate, Ca++ |
| potassium sparing diuretics | amiloride and spironolactone |
| ACEi/ARB | Fall in BP Rise in K+ Rise in creatinine Renal artery stenosis Fall in Hb Side effects - cough, rash, angio-oedema |
| PPT notes on arrhythmias | Lignocaine, class Ib, used for VT/VF, IV only Flecainide, class Ic, used for SVT/AF Sotalol - betablocker with class III activity, used for AF prophylaxis Betablockers - AF prophylaxis, SVT prophylaxis, VT prophylaxis Adenosine - blocks AV node conduction and arrests SVT verpamil, class IV, arrest SVT |
| amiodarone side effects | hyper/po - thyroidism photosensitivity with grey blue discolouration Corneal microdeposits Peripheral neuropathy Hepatic damage Pulmonary fibrosis |
| Digoxin | controls ventricular rate in AF Dangers of hypokalaemia digibind |
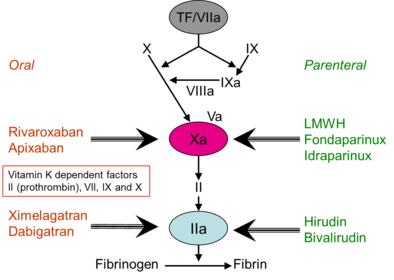
| Warfarin | Inhibits the reduction of vitamin K therefore the production of the relevant clotting factors - II, VII, IX, X |
| who to anticoagulate | CHA2DS2VASc - stroke risk in AFib |
| newer anticaogulants | |
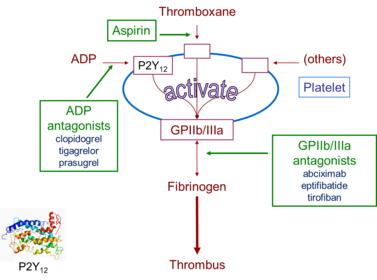
| antiplatelets | |
| Clinical used of antiplatelets | |
| Dopamine theory in schizophrenia | Dopamine neuron under active in prefrontal cortex (negative symptoms of schizophrenia) and release of mesolimbic dopamine neurons from inhibitory control (positive symptoms of schizophrenia) |
| drugs used post MI | Beta-adrenoceptor antagonists Angiotensin converting enzyme inhibitors HMGCoA antagonists (statins) Antithrombotic therapy Antiplatelet |
| 1st vs 2nd gen antipsychotics | 2nd gen work on 5ht2 receptors also (except amisulpiride) More likely to cause weight gain, diabetes and dyslipidaemia. less likely to have extrapyramidal side effects |
| Aripiprazole | Partial agonist at D2 receptors hence potential to improve negative symptoms Significantly better side effect profile except for high incidence of akathisia (physical and mental restlessness with urges to move about) |
| treatment resistant schizophrenia | Clozapine Combining medications CBT Family Therapy |
| Treatment of bipolar | |
| Mood stabilisers | Lithium Antiepileptics ( Valproate, carbamazepine, lamotrigine) Antipsychotics (such as quetiapine) Benzodiazepines |
| depression treatment resistance | Review diagnosis Look at comorbid physical illnesses Change antidepressant Augment Lithium Lamotrigine Antidepressant Antipsychotics |
| Venlafaxine and duloxetine | SNRIs Dual acting but better tolerated than TCAs Generally 2nd line treatment Duloxtine licensed for chronic pain, stress incontinence and for diabetic neuropathy. |
| NaSSA | Mirtazapine- ‘broad spectrum antidepressant’ Side effects: sedation, weight-gain, metabolic syndrome |
| MAO-I | Reversible - Moclobomide Irreversible – phenelzine, tranylcipromine Dietary restrictions |
| What to do in TCA overdose | Overdose --> wide QRS --> sodium bicarbonate --> QRS back to normal supportive ECG monitoring serial 12-lead ECGs IV bicarbonate if at risk consider IV magnesium |
| when to use acetylcysteine | Above ‘100-line’ (0-15 hours) No need to consider ‘risk factors’ Close to limit of detection >15 hours (late) paracetamol overdose and staggered intake or over 15 hours then can't use normogram have to then rely on dose <75 mg/kg toxicity unlikely 75-150 mg/kg toxicity possible >150 mg/kg toxicity likely |
| What can you get in acetylcystein | non-IgE anaphylactic reactions Flushing, hypotension, rash, wheeze |
| Charcoal | if within 1 hour, airway risk of aspiration, avoid in intestinal obstruction |
| Multiplke dose axctivated charcoaal in what | Carbamazepine Quinine Theophylline Phenobarbitone |
| Drugs not absorbed by activated charcoal | Ethanol Ethylene glycol Iron Lithium Methanol |
| Guidelines on order of neuropathic pain meds | National Institute of Clinical Excellence (UK) guidelines: First line: Amitriptyline (Imipramine if cannot tolerate) or pregabalin Second line: Amitriptyline AND pregabalin Third line: refer to pain specialist. Give tramadol in the interim (avoid morphine) If diabetic neuropathic pain: Duloxetine |
| UTI, what drug to avoid | Quinolones such as ciprofloxacin and levofloxacin - lower the seizure threshold |
| Tuberculosis drugs MOA and side effects | Rifampicin mechanism of action: inhibits bacterial DNA dependent RNA polymerase preventing transcription of DNA into mRNA potent liver enzyme inducer hepatitis, orange secretions flu-like symptoms Isoniazid mechanism of action: inhibits mycolic acid synthesis peripheral neuropathy: prevent with pyridoxine (Vitamin B6) hepatitis, agranulocytosis liver enzyme inhibitor Pyrazinamide mechanism of action: converted by pyrazinamidase into pyrazinoic acid which in turn inhibits fatty acid synthase (FAS) I hyperuricaemia causing gout arthralgia, myalgia hepatitis Ethambutol mechanism of action: inhibits the enzyme arabinosyl transferase which polymerizes arabinose into arabinan optic neuritis: check visual acuity before and during treatment dose needs adjusting in patients with renal impairment |
| eye drops to anaesthetise the eye | best ones - proxymetacaine and oyxbruprocaine less good - tetracaine |
| Short acting drug use to diagnose myasthenia gravis | edrophonium Additional info: -immunological treatment - prednisolone or azathioprine -plasmapheresis in which blood is removed and the cells returned, may improve motor function, presumably reduces immune complexes - thymectomy may be curative |
| side effects of competitive neuromuscular blocking drugs | Pancuronium - tachycardia Vercuronium - no CV effects Atracurium - good in renal and hepatic impairment, causes histamine release with flushing and hypotension Cisatracurium - does not cause histamine release and the associated side effects Rocuronium - minimal CV effects |
| Name of the depolarising neuromuscular blocking drug and its main disadvantage | Suxamethonium main disadvantage - initial asynchronous muscle fibre twitches cause damage and subsequent muscle pains. damage also releases potassium repeated doses may cause bradycardia |
| What drug to use in BPH and how does it work | Tamsulosin an alpha1A adrenoreceptor antagonist, relaxes smooth muscle in the prostate gland |
| Drugs that decrease IOP by increasing outflow | Latanoprost (a prostaglandin that increases uveoscleral outflow of aqueous) Pilocarpine (muscarinic agonist which, contracts the ciliary muscle --> trabecular meshwork stretched and separated --> fluid pathways opened up and aqueous outflow increased. -side effects - miosis, poor night vision, headache, brow ache. |
| Drugs that reduce IOP by decreasing aqueous secretion other than B blocker | Brominidine and apraclonidine are A2-adrenoreceptor agonists. They decrease aqueous formation by stimulating A2-receptors on the adrenergic nerve terminals innervating the ciliary body (thus reducing norepinephrine release) Carbonic anhydrase inhibitors - Acetazolamide - acts on ciliary body and prevent bicarbonate synthesis --> fall in sodium transport and aqueous formation because bicarbonate and sodium transport are linked - oral or IV - too toxic for long term use. -Dorzolamide -a sulphonamide and systemic side-effects may occur, e.g. skin rashes, bronchospasm Laser trabecular surgery - can use as alternative to drugs. create about 100 lesions on the inner surface of the trabecular meshwork --> causes localised shrinkage --> tension on untreated tissue --> opens spaces in the meshwork allowing increased aqueous drainage |
| drugs to treat wet age released macular degeneration | Verteporfin - a photosensitive dye that is combined with photodynamic therapy. anti-VEGF Mabs - bevacizumab, pegaptanib, ranibizumab |
| Side effects of theophylline | nausea, headache, insomnia and abdominal discomfort common, even in therapeutic ranges 10-20mg/l above 25mg/l toxic effects include serious arrhythmias. |
| which histamine in allergy and which in GI | H1 allergy H2 GI (e.g. parietal cell stimulation) |
| Which GI drug can cause gynaecomastia and can bind to cytochrome -450 to reduce metabolism of warfarin, phenytoin and theophylline | Cimetidine |
| example peptic ulcer disease regimes | Clrithromycin, omeprazole and metronidazole Or if not clarithromycin then amoxicillin. |
| name the 4 types of laxative, give examples and how they work | Bulk laxatives - isphagula, bran - increase volume of intestinal contents to stimulate peristalsis osmotic laxatives - increase bulk of the bowel by retaining water - MgSO4, lactulose, movicol Stimulant laxatives - increase motility by acting on the mucosa or the nerve plexuses, which may be damaged by prolonged drug use - senna, bisacodyl and sodium picosulphate (mainly to evacuate bowel before surgery), docusate, glycerol suppositories Faecal softeners - promote defection by softening (e.g. docusate) and/or lubricating (e.g. arches oil) faeces |
| ulcerative colitis vs Crohn's - inducing remission and maintenance | UC and Crohn's remission - rectal (topical) aminosalicylates or steroids: oral aminosalicylates oral/IV prednisolone Crohn's remission cont - azathioprine and mercaptopurine can be added on. -can use methotrexate -infliximab in fistulating and recurrent disease -metronidazole for isolated peri-anal disease Maintenance UC: mesalazine. can also use mercaptopurine and azathioprine (both are first line in Crohn's) Crohn's second line maintenance - methotrexate -can also consider mesalazine if had surgery assess thiopurine methyltransferase (TPMT) activity before offering azathioprine or mercaptopurine |
| side effects of bendroflumethiazide | Common or very common Altered plasma-lipid concentrations; gout; hypercalcaemia; hyperglycaemia; hyperuricaemia; hypochloraemic alkalosis; hypokalaemia; hypomagnesaemia; hyponatraemia; metabolic and electrolyte disturbances; mild gastrointestinal disturbances; postural hypotension |
| In renal impairment, which of thiazides or loop diuretics are effective | thiazides ineffective when eGFR less than 30 Loop still effective. |
| side effects of loop diuretics | hyponatraemia, hypotension, hypovolaemia, and hypokalaemia, hypomagnesaemia rapid IV can cause deafness which may not be reversible |
| names of K+ sparing diuretics, MOA, side effects | Spironolactone - competitive antagonist of aldosterone - can cause sever hyperkalaemia esp in renal impairment, also likely to occur if taking ACEi as these drugs reduce aldosterone secretion Amiloride and triamterene - blocks the sodium channels, which increases Na excretion and decreases K+ excretion |
| a good cardioselective beta blocker to use in hypertension | atenolol |
| management of acute severe hypertension | use oral drugs first e.g. atenolol and amlodipine Hydrazine (IV), labetalol (oral or IV), nifedipine (oral) in hypertension associated with eclampsia Magnesium sulphate to prevent fits. |
| Side effects of nitrates | headaches, hypotension, fainting - due to arteriolar vasodilation reflex tachycardia but can prevent with B blocker prolonged high dosage may cause methaemoglobinaemia |
| pharmacological management of bradycardia post MI | ABCDE ECG atropine could use procainamide ? may need some form of pacing |
| Drugs used in supra ventricular arrhythmias | Adenosine - slows conduction in the AVN, short lived side effects of dyspnoea, bronchospasm, feel awful. --> paroxysmal SVT Digoxin - delays AV conduction, increases degree of block and strengthens the ventricular beat IV used --> uncontrolled a flutter and fibrillation Verapamil - largely replaced by adenosine as it is safer, especially if patient has a VT in which case verapamil would be very bad. orally used for prophylaxis of SVT Should not use with B blockers or quinidine because of cumulative negative inotropic effects |
| Drugs effective in SVT and Ventricular arrhythmias | Class IA agents: block voltage dependent Na channels -Disopyramide - mainly used orally to prevent recurrent ventricular arrhythmias. Negative inotropic action , may cause hypotension (especially IV )and aggravate cardiac failure. Also causes nausea and vomiting, anticholinergic effects such as urinary retention -Procainamide - similar but has less antimuscarinic action Class IC -flecainide - strongly depress conduction in myocardium, mainly used in prophylaxis of paroxysmal AF, but has negative inotropic action and may cause ventricular arrhythmias, esp after MI Class III agents -acts by slowing depolarisation and prolonging the action potential and refractory period in all cardiac tissues -amiodarone - blocking actions on K+ and inactivated Na channels) and B adrenoreceptors. often effective when other drugs have failed but long term use restricted by things like photosensitivity, thyroid disorders, neuropathy and pulmonary alveolitis -Sotalol - class III and II (B blocking) actions. lacks the side effects of amiodarone but has usual side effects of B blockers |
| Drugs used in ventricular arrhythmias | class IB agents -block inactivated voltage dependent Na channels -Lidocaine IV - ventricular arrhythmias, usually after acute MI - has little effect on normal cardiac tissue but in ischaemic areas where anoxia causes depolarisation and arrhythmigenic activity, many Na+ channels are inactivated and therefore susceptible to lidocaine. |
| How to assess cardiovascular risk How to reduce also | QRISK2 to assess Lifestyle modifications to reduce risk: -diet in which total fat intake is 30% or less of total energy intake, saturated fats are 7% or less of total energy intake, intake of dietary cholesterol is less than 300 mg/day and where possible saturated fats are replaced by mono‑unsaturated and polyunsaturated fats. -choose wholegrain varieties of starchy food -reduce their intake of sugar and food products containing refined sugars including fructose -eat at least 5 portions of fruit and vegetables per day -eat at least 2 portions of fish per week, including a portion of oily fish -eat at least 4 to 5 portions of unsalted nuts, seeds and legumes per week. at least 150 minutes of moderate intensity aerobic activity or 75 minutes of vigorous intensity aerobic activity or a mix of moderate and vigorous aerobic activity Manage obesity alcohol guidelines Stop smoking Salt for hypertension Lipid modification therapy - |
| Which classes (and give examples of drugs) can be used to reduce nausea and vomiting of motion sickness | Antimuscarinic drugs - hyoscine Antihistamines - cinnarizine, promethazine, cyclizine |
| How to treat vertigo and vomiting associated with vestibular disease | Antihistamines e.g. promethazine, cinnarizine phenothiazines (e.g. prochlorperazine) or betahistine |
| Good combination of drugs to prevent chemo induced emesis | Metoclopramide or Ondansetron With - dexamethasone Ondansetron is also classically used for antiemesis in chemo drugs. |
| Specific antiemetic to use in Meniere's disease | Betahistine - supposed to act by reducing endolymphatic pressure |
| name the 2 classes of steroid hormones, examples and where they are made | mineralocorticoids - mainly aldosterone, salt retaining activity, synthesised in the cells of zona glomerulosa glucocorticoids - mainly cortisol (hydrocortisone), affects carbohydrate and protein metabolism. but also significant mineralocorticoid activity. synthesised in cells of zona fasciculata and zona reticularis |
| What types of insulin are these: Insulin deter, Insulin glargine | Long acting OD |
| What type of insulin is isophane insulin | Intermediate acting |
| What type of insulins are these: Insulin lispro, insulin apart, insulin glulisine | Short acting Soluble insulin is also part of this |
| What is co-trimoxazole? and a specific bacteria is is good with | combination of trimethoprim and sulfamethoxazole may produce a synergistic action Pneumocystis jiroveci, nocardiasis and toxoplasmosis |
| good drug to use for analgesia when you want to avoid morphine associated sphincter spasm | pethidine |
| give examples of GnRH agonists, what they are used in and how they work | Zoladex (goserelin acetate) and Prostap (leuprorelin acetate) Agonists bind to GnRH receptors and produce an initial intense stimulation. This causes marked increases in LH, FSH and testosterone/oestrogen. Sustained pituitary overstimulation will eventually down-regulate/desensitize GnRH receptors with a consequent decrease in hormone levels Prostate cancer, breast cancer, endometriosis, reduce size of fibroids prior to surgery |
| Which two conditions is clopidogrel first line anti platelet therapy for | Ischaemic stroke and peripheral vascular disease |
| who should receive a statin | established cardiovascular disease (stroke, TIA, ischaemic heart disease, peripheral arterial disease) 10 year cardiovascular risk |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quer criar seus próprios Flashcards gratuitos com GoConqr? Saiba mais.