6491376
Descrição
FlashCards por Andrew Street, atualizado more than 1 year ago
|
|
Criado por Andrew Street
mais de 8 anos atrás
|
|
| Questão | Responda |
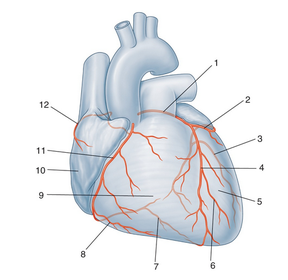
| 960 Name the arteries & anatomical regions. | |
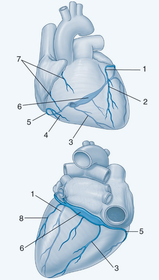
| 960 Name the veins. | |
| 961 S & Sx of angina. | * Central chest tightness, heaviness, or P. May be mild-severe. Bought on by exertion & relieved by rest. Other precipitants may be cold weather, emotion, heavy meals. * Associated Sx inc dyspnoea, nausea, sweatiness, faintness, fear. OHCM p111. |
| 962 DDx for chest P. | * CVS: > Angina > MI > Acute aortic dissection > Pericarditis * GI: > Reflux oesophagitis > Peptic ulcer DS > Oesophageal spasm * Pulmonary: > Pneumonia > Pneumothorax > PE * Musculoskeletal: > Chest wall injuries > Herpes zoster > Costochondritis > Secondary tumours of the rib. DDx p57. |
| 964 List risk factors for developing CAD. | |
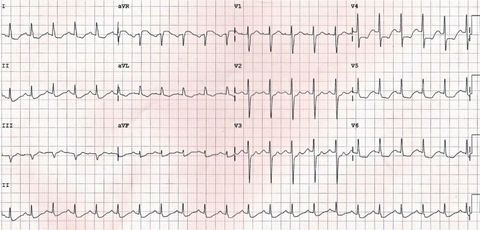
| 965 Which ECG change is seen that is associated with myocardial ischaemia? | ST depression due to myocardial ischaemia may be present in a variable number of leads and with variable morphology. In this eg - widespread subendocardial ischaemia due to LMCA occlusion. http://lifeinthefastlane.com/ecg-library/myocardial-ischaemia/ |
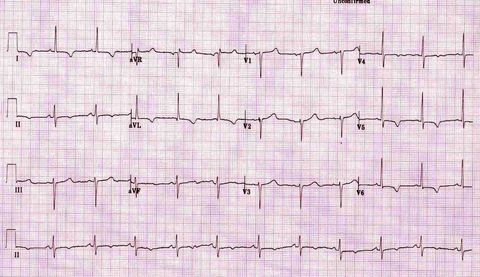
| 965 Which ECG change is seen that is associated with myocardial ischaemia? | T wave inversion may be considered to be evidence of myocardial ischaemia if: * At least 1 mm deep * Present in ≥ 2 continuous leads that have dominant R waves (R/S ratio > 1) * Dynamic — not present on old ECG or changing over time. In this eg - widespread T wave inversion due to myocardial ischaemia (most prominent in the lateral leads). http://lifeinthefastlane.com/ecg-library/myocardial-ischaemia/ NB. T wave inversion is only significant if seen in leads with upright QRS complexes (dominant R waves). T wave inversion is a normal variant in leads III, aVR and V1. |
| 965 Describe Ix that can be used to confirm the diagnosis of angina. | * Known CAD & P typical then no further Ix * Known CAD & atypical P then either exercise testing or functional imaging * Unknown CAD - stratify likelihood of CAD • >90% treat as known CAD • 61–90% angiography, or functional imaging if inappropriate • 30–60% functional imaging • 10–29% coronary artery calcification score with CT • <10% reconsider Dx. See note 'Calculating the Likelihood of CAD'. http://oxfordmedicine.com/view/10.1093/med/9780199609628.001.0001/med-9780199609628-chapter-3#med-9780199609628-chapter-3-div1-12 |
| 966 Discuss the non-pharmacological Mx of stable angina. | Modify risk factors: * Stop smoking * ^Exercise * Weight loss * Control HT * Good Mx of DM * If ^total cholesterol give a statin. OHCM p110. |
| 967 What are the classes of drugs used to Rx stable angina? | * Anti-platelet Rx - aspirin * Anti-anginal Rx - 1st line Rx is beta-blockade, 2nd is calcium channel blocker * Statin or other lipid-lowering Rx - primary option is artorvastatin * Anti-hypertensive Rx - primary option is a beta-blocker &/or an ACEi. From BMJ Best Practice. http://bestpractice.bmj.com/best-practice/monograph/148/treatment/details.html |
| 968 Explain to a pt how to take sublingual GTN in the event of chest P. | Spray one or two sprays under your tongue when a P develops. Close your mouth immediately after using the spray. Your pain should ease within a minute or so. If the first dose does not work, use the spray again after five minutes. If the pain continues for 15 minutes despite using the spray twice then call an ambulance straightaway. http://patient.info/medicine/glyceryl-trinitrate-for-angina-gtn |
| 970 Why is cardiac catheterization performed & what are the complications? | Uses: * To sample BD to asses O2 sats & measure pressures * To inject radiopaque contrast * Tp perform angioplasty (+/- stenting), valvuloplasty, cardiac biopsies, other procedures such as ASD closure * Intravascular US or echocardiography Complications: * Haemorrhage * Contarst reaction * Loss of peripheral pulse - due to dissection, thrombosis, arterial spasm * Angina * Arrhythmias * Tamponade * Infxn * Mortality - <1:1000 in most centres. OHCM p104. |
| 971 Discuss indications for coronary artery bypass surgery. | CABG is performed in L main stem DS, multi-vessel DS; multiple severe stenoses; pt's unsuitable for angioplasty; failed angioplasty; refractory angina. Indications for CABG: * To ^survival in - • L main stem DS • Triple vessel DS involving proximal part of the LAD * To relieve Sx in - • Angina unresponsive to drugs • Unstable angina (sometimes) • If angioplasty is unsuccessful. OHCM p117. |
| 977 Outline the pathology of atheroma. | |
| 979 Outline the pathogenesis of coronary thrombus formation. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quer criar seus próprios Flashcards gratuitos com GoConqr? Saiba mais.