326681
Beschreibung
Mindmap von melian.yates, aktualisiert more than 1 year ago
|
|
Erstellt von melian.yates
vor etwa 11 Jahre
|
|
Liver
Pathology
- Functions
- Portal Vein
- Metabolic
processing
- Dietary
carbohydrates
- Lipids
- Amino Acids
- Vitamins
- Vitamins
- Amino Acids
- Lipids
- Dietary
carbohydrates
- Detoxification,
Degredation &/or
Biliary Excretion
- Endogenous
wastes
- Toxic
molecules
- Hormones
- Xenobiotic
compounds
- Biotransformation
of drugs
- Biotransformation
of drugs
- Xenobiotic
compounds
- Detoxified chemical
wastes
- Hormones
- Bile salts,
Bilirubin,
cholesterol,
HCO3-, H2O
- Toxic
molecules
- Endogenous
wastes
- Blood from
Intestinal tract
- Processing &
Activation of
some xenobiotic
agents
- Pro-drugs
- Ex. Cytochrome
p450
- Ex. Cytochrome
p450
- Pro-drugs
- Metabolic
processing
- Synthesis of Plasma Proteins
- Albumin
- Globulins
- Clotting
factors
- Complement
proteins
- Clotting
factors
- Other serum
transport/ binding
proteins
- Globulins
- Albumin
- Storage
- Glycogen
- Fats
- Fe
- Cu
- Vitamins
- Ex. Vitamin A
(stored in Hepatic
stellate cells)
- Ex. Vitamin A
(stored in Hepatic
stellate cells)
- Vitamins
- Cu
- Fe
- Fats
- Glycogen
- Processing of Vitamin D
- With Kidneys
- With Kidneys
- Removal of Bacteria & Erythrocytes
- Kupffer cells
- Removal of
Erythrocytes also
occurs in the
Spleen
- Kupffer cells
- Portal Vein
- Clinical Signs of Liver Disease
- Jaundice/
Icterus
- Accumulation of bilirubin in the body
- Mechanism
- Pre-Hepatic
- Excessive
breakdown of
Erythrocytes
- Liver is overwhelmed
& cannot excrete the
bilirubin fast enough
- Ex. IMHA (Immune
mediated
Haemolytic
Anaemia)
- Ex. IMHA (Immune
mediated
Haemolytic
Anaemia)
- Liver is overwhelmed
& cannot excrete the
bilirubin fast enough
- Excessive
breakdown of
Erythrocytes
- Post-Hepatic
- Physical obstruction
of bile outflow
- Damage, disease,
compression or
obstruction of the
gallbladder or
common bile duct
- Prevents Bile from
being excreted into the
small intestine
(Cholestasis)
- Ex. Gallstones,
compressive tumor
- Ex. Gallstones,
compressive tumor
- Prevents Bile from
being excreted into the
small intestine
(Cholestasis)
- Damage, disease,
compression or
obstruction of the
gallbladder or
common bile duct
- Physical obstruction
of bile outflow
- Hepatic
- Liver is diseased
& cannot excrete
even the normal
bilirubin load
- Ex. Cirrhosis
- Ex. Cirrhosis
- Liver is diseased
& cannot excrete
even the normal
bilirubin load
- Pre-Hepatic
- Accumulation of bilirubin in the body
- Oedema/Ascites/Anasarca
- If the liver is unable to
synthesize the normal
plasma proteins, there will
be a reduction in plasma
oncotic pressure
- Ex. Decrease in serum
Albumin, Decrease in
Oncotic pressure
- Fluid moves out of
circulation => Fluid
accumulates in the body
cavities & subcutaneous
spaces
- Ex. Decrease in serum
Albumin, Decrease in
Oncotic pressure
- If the liver is unable to
synthesize the normal
plasma proteins, there will
be a reduction in plasma
oncotic pressure
- Coagulation (Clotting)
Disorders
- If liver is unable to produce
sufficient clotting factors,
fibrinolytic proteins,
complement proteins &
acute phase proteins:
- => Poor or inappropriate
Haemostasis & immune function
- Risk of
Haemorrhage after
liver biopsy
- Paradoxial balance
- Liver products
- Pro-coagulation
- Lack of Anti-clotting factors
- Lack of Anti-clotting factors
- Anti-coagulation
- Lack of clotting factors
- Lack of clotting factors
- Pro-coagulation
- Liver products
- Risk of
Haemorrhage after
liver biopsy
- => Poor or inappropriate
Haemostasis & immune function
- If liver is unable to produce
sufficient clotting factors,
fibrinolytic proteins,
complement proteins &
acute phase proteins:
- Hepatic Encephalopathy
- Liver usually converts ammonia
into urea (excreted by the kidneys)
- NH3 produced
in intestine by
bacteria
- NH3 produced
in intestine by
bacteria
- Liver disease:
- Reduced ability to
detoxify &/or remove
nitrogenous compounds
from the body
- Increased [NH3] &
other toxic
substances (Mn?) in
the blood
- => Impairs brain function
- =>Status spongiosus of
white matter in CNS
- Multiple fluid filled spaces
of microscopic size in
cerebral white matter
- Multiple fluid filled spaces
of microscopic size in
cerebral white matter
- =>Status spongiosus of
white matter in CNS
- Toxicity
- => Impairs brain function
- Increased [NH3] &
other toxic
substances (Mn?) in
the blood
- Reduced ability to
detoxify &/or remove
nitrogenous compounds
from the body
- Liver usually converts ammonia
into urea (excreted by the kidneys)
- Metabolic disease & dysfunction
- Liver disease (Reduced ability to):
- Process dietary
components delivered
from the portal blood
- Store Glycogen, fat &
vitamins
- Detoxify endogenous or exogenous
toxins
- Implications for drug
selection, administration &
dosage
- Process dietary
components delivered
from the portal blood
- Liver disease (Reduced ability to):
- Jaundice/
Icterus
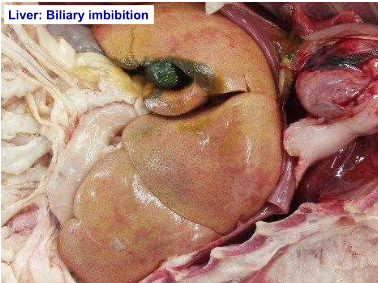
- Incidental Post-Mortem
Changes
- Prone to rapid PM
change:
- Composition
- Vascularity
- Proximity to the intestine
- Proximity to the intestine
- Vascularity
- Composition
- Softening & increased
friability
- Production of gas bubbles
(Putrefactive bacterial
fermentation)
- Black discoloration
(bacterial breakdown
of Hb)
- Green discoloration (Bile
leakage)
- Biliary
Imbibition
- Biliary
Imbibition
- Microscopically:
- Dissociation of hepatocyte
cords
- Pyknosis of
nuclei
- Lysis of
hepatocytes
- Lysis of
hepatocytes
- Pyknosis of
nuclei
- Dissociation of hepatocyte
cords
- Prone to rapid PM
change:
- Hepatic Degeneration
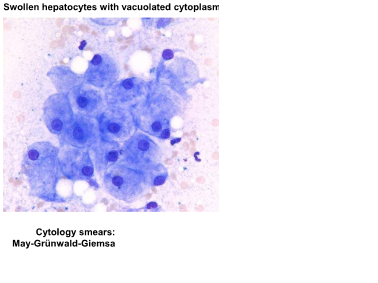
- Hydrophobic Degeneration (Cloudy swelling)
- Hepatocellular swelling
- Early manifestation of cell
injury (Hypoxia, toxins)
- Hepatocytes unable
to maintain normal
homeostatsis
- NRG production
decreases => membrane
pumps fail => lack of ATP
- Intracellular accumulation
of H2O
- Swelling of mitochondria
& other organelles
- Swelling of mitochondria
& other organelles
- Intracellular accumulation
of H2O
- NRG production
decreases => membrane
pumps fail => lack of ATP
- Hepatocytes unable
to maintain normal
homeostatsis
- Cytoplasmic vacuoles
may develop if severe
- Early manifestation of cell
injury (Hypoxia, toxins)
- Reversible
- Hepatocytes not
damaged or
destroyed
- Hepatocytes not
damaged or
destroyed
- Hepatocellular swelling
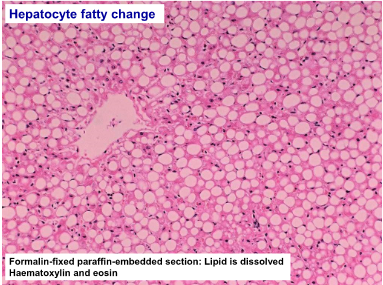
- Fatty Change
- Lipid accumulates in
cytoplasm of injured
hepatocytes
- Inability to
metabolize/function normally
(Hypoxia, toxins)
- I.e. Conversion of
FFA => TAG
- I.e. Conversion of
FFA => TAG
- Often more severe
damage than in hydropic
degeneration/cloudy
swelling
- Reversible (If inciting
cause is
removed/corrected)
- Fatty change (due to
hypoxia/toxins) may
eventually lead to
lipidosis/steatosis when
severe &/or chronic
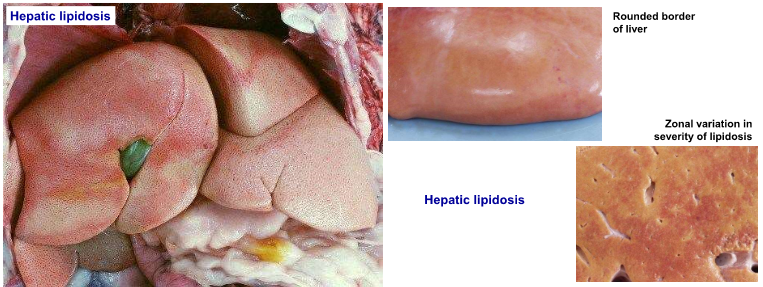
- Hepatic Lipidosis/Steatosis
- Hepatocytes distended by
discrete circular lipid vacuoles
(displace nucleus to periphery
of cell)
- Due to massive uptake of fatty acids
from the bloodstream following
excessive mobilisation of adipose
tissue reserves => Overloads
metabolic capacity of hepatocytes &
further inhibits their function
- Hepatocytes distended by
discrete circular lipid vacuoles
(displace nucleus to periphery
of cell)
- Pale, yellow,
friable,
"greasy" liver
- Causes:
- Starvation
- Equine
hyperlipaemia
- Negative NRG
balance in
cattle
- Feline hepatic
lipidosis
- Feline
hyperlipaema
- Diabetes mellitus (Glycogen vs.
lipid)
- Hypoxia/toxins =>
Lipidosis
- Hypoxia/toxins =>
Lipidosis
- Diabetes mellitus (Glycogen vs.
lipid)
- Feline
hyperlipaema
- Feline hepatic
lipidosis
- Negative NRG
balance in
cattle
- Equine
hyperlipaemia
- Starvation
- Lipid accumulates in
cytoplasm of injured
hepatocytes
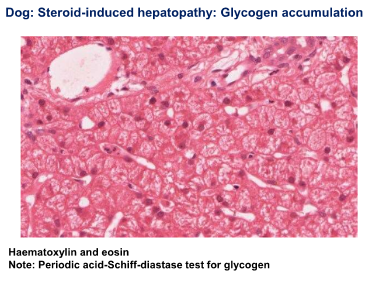
- Glycogen (Steroid Induced Hepatopathy)
- Excessive
accumulation of
glycogen in the
presence of high levels
of corticosteroids
- Exogenous corticosteroids
- E.g.
Dexamethasone
(iatrogenic)
- E.g.
Dexamethasone
(iatrogenic)
- Endogenous corticosteroids
- Hyperadrenocorticism
- Diabetes mellitus
- Glycgoen &/or fat
accumulations
- Glycgoen &/or fat
accumulations
- Diabetes mellitus
- Hyperadrenocorticism
- Exogenous corticosteroids
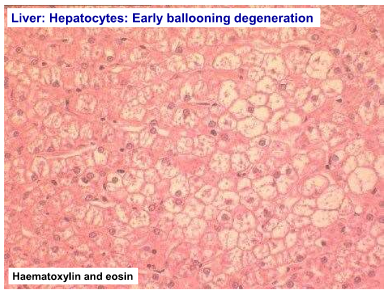
- Hepatocytes distended by
floccular ("feathery")
cytoplasmic vacuoles (do not
displace the nucleus)
- Ballooning
degeneration
may occur
- Irreversible
- Irreversible
- Excessive
accumulation of
glycogen in the
presence of high levels
of corticosteroids
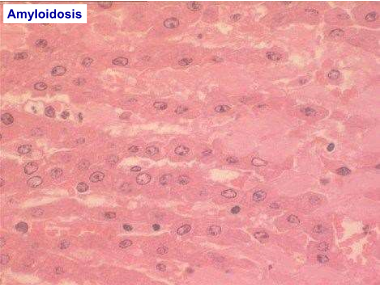
- Amyloidosis
- Primary
- Can be familial
- Shar pei dogs
- Abyssinian,
Siamese & other
exotic cats
- Can be familial
- Secondary
- Chronic inflammation
- Chronic inflammation
- Gross pathology
- Liver is enlarged
- Pale & firm
- Rounded
borders
- Rounded
borders
- Pale & firm
- Liver is enlarged
- Histopathology
- Amyloid is deposited
extracellularly around portal
tracts & along sinusoids in
the space of Disse
- Can also be
deposited in
kidneys, pancreas,
blood vessels
- Can also be
deposited in
kidneys, pancreas,
blood vessels
- Amyloid is deposited
extracellularly around portal
tracts & along sinusoids in
the space of Disse
- Special stains
- Congo red +
Green
birefringence
- Congo red +
Green
birefringence
- Types:
- AA Type
- Derived from the
inflammatory acute phase
protein serum amyloid A
- Derived from the
inflammatory acute phase
protein serum amyloid A
- AL Type
- Derived from Ig light chains
- Derived from Ig light chains
- ABeta type
- Derived from amyloid precursor protein &
islet amyloid polypeptide (IAPP: Hormone
produced by Beta cells in pancreatic islets
of cats)
- Derived from amyloid precursor protein &
islet amyloid polypeptide (IAPP: Hormone
produced by Beta cells in pancreatic islets
of cats)
- AA Type
- Primary
- Hydrophobic Degeneration (Cloudy swelling)
- Hepatic
Necrosis
- Mode of action of agent
- Directly affects
hepatocellular or
biliary cells
- Secondary to
interference with
blood supply or
biliary tract
damage
- Directly affects
hepatocellular or
biliary cells
- Severity & duration of action of
agent
- Mild &/or short
duration => Reversible
change
- Severe, constant or
repeated action =>
Irreversible change
- Mild &/or short
duration => Reversible
change
- Route of Access of
Agent
- Umbilical vein in
foetus/neonate
- Portal Vein
- Hepatic Artery
(O2)
- Transcoelemic
- Infections,
neoplasms
- Biliary
system
- Ascending
infections
- Ascending
infections
- Infections,
neoplasms
- Toxins
- Transcoelemic
- Hepatic Artery
(O2)
- Portal Vein
- Umbilical vein in
foetus/neonate
- Single-Cell Necrosis
- Coagulative necrosis of
individual cells & their
immediate neighbors
- Some forms of viral
hepatitis e.g. Herpesvirus
- Coagulative necrosis of
individual cells & their
immediate neighbors
- Focal
Necrosis
- Usually a microscopic change
in hepatocytes/biliary cells
randomly distributed without
obvious relationship to
lobular pattern
- Can be of minimal clinical
significance
- Viral & bacterial agents most
common
- Usually a microscopic change
in hepatocytes/biliary cells
randomly distributed without
obvious relationship to
lobular pattern
- Zonal Necrosis
- Centrilobular (Periacinar)
Necrosis
- Hepatocytes are vulnerable to
Hypoxic damage (Chronic
venous congestion; Anaemia) b/c
of relatively low gradient of O2
in center of the lobule
- Also susceptible to
toxic insult by
toxins requiring
hepatic
biotransformation
- Also susceptible to
toxic insult by
toxins requiring
hepatic
biotransformation
- Hepatocytes are vulnerable to
Hypoxic damage (Chronic
venous congestion; Anaemia) b/c
of relatively low gradient of O2
in center of the lobule
- Most common
- Periportal
Necrosis
- Commonly seen in toxic
damage where the toxin is
preformed (closest to the
incoming blood supply)
- Portal vein
or Hepatic
artery
- Portal vein
or Hepatic
artery
- Commonly seen in toxic
damage where the toxin is
preformed (closest to the
incoming blood supply)
- Centrilobular (Periacinar)
Necrosis
- Massive Necrosis
- Complete necrosis of
individual lobules
(cells & connective
tissue scaffold)
- May be isolated or
multiple lobules
- More Serious insult
&/or longer duration
insult
- Does not
neccessarily
mean whole organ
is affected
- Followed by
"Post-necrotic lobular
collapse" & fibrosis
(due to loss of reticulin
scaffold
- Ex. Hepatosis
dietica (Vit. E
deficiency - Pigs)
- Complete necrosis of
individual lobules
(cells & connective
tissue scaffold)
- Mode of action of agent
- Response of Liver to
Inflammation
- Hypertrophy of Hepatocytes
- Increase in size of surviving
Hepatocytes: Increased
amount of cytoplasm
- Increase in size of surviving
Hepatocytes: Increased
amount of cytoplasm
- Regenerative Hyperplasia
- Nodular regeneration of
existing mature hepatocytes
in response to liver injury
- Ability to
regenerate
varies w/
species & age
- Ability to
regenerate
varies w/
species & age
- Hyperplasia may
be diffuse, but
often occurs as:
- Microscopic nodules
(Micronodular
Hyperplasia)
- Macroscopic nodules
(Macronodular
hyperplasia)
- Microscopic nodules
(Micronodular
Hyperplasia)
- Nodular regeneration of
existing mature hepatocytes
in response to liver injury
- Nodular
Hyperplasia
- Common incidental
finding in older dogs
- Discrete, unencapsulated
nodules of hepatocytes which
retain good architecture of
hepatic lobules & hepatocyte
cords
- Might be
slightly
vaculated
- Might be
slightly
vaculated
- No evidence of
concurrent hepatic
disease
- Not inflammatory
- Needs to be differentiated
from macronodular
regeneration & neoplasia
- Needs to be differentiated
from macronodular
regeneration & neoplasia
- Common incidental
finding in older dogs
- Oval Cell Proliferation
- Regeneration of new
hepatocytes & bile ducts by
proliferation of bipotential stem
cells ("Oval cells") located in
the terminal bile ductules
(canals of Hering)
- Oval cells =
source of Hepatic
Fibrosis
- Often just see
proliferation of bile duct
type cells
- i.e. more differentiated
cells => biliary
hyperplasia
- i.e. more differentiated
cells => biliary
hyperplasia
- Oval cells =
source of Hepatic
Fibrosis
- Regeneration of new
hepatocytes & bile ducts by
proliferation of bipotential stem
cells ("Oval cells") located in
the terminal bile ductules
(canals of Hering)
- Hepatic Atrophy
- Atrophy of the whole liver,
individual lobes or parts of
lobes
- Pressure on liver
parenchyma, e.g. External or
internal space occupying
lesions
- Anoxia/Hypoxia (Insidious
O2 deprivation)
- Impairment of bile flow:
Chronic biliary disease
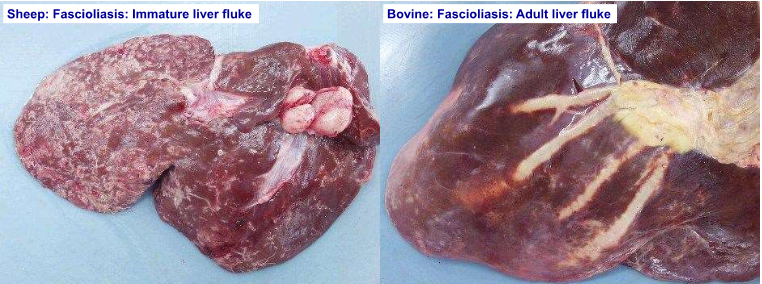
- Fasciola hepatica
infestation (Cattle &
Sheep)
- Cholestasis (Dogs & Cats)
- Fasciola hepatica
infestation (Cattle &
Sheep)
- Atrophy of the whole liver,
individual lobes or parts of
lobes
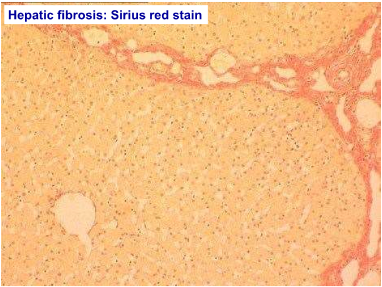
- Fibrosis
- Localized or generalized
deposition of extracellular
connective tissue matrix
(fibrous/scar tissue) as a healing
response to hepatic injury
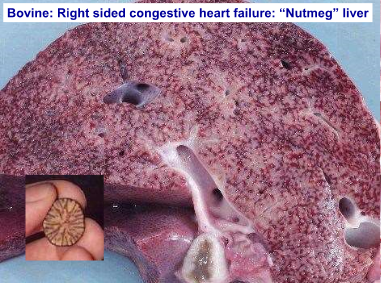
- Centrilobular fibrosis
- Prolonged hypoxia, cell
death & fibrosis of
centrilobular zones
- Chronic venous
congestion
(Cardiac failure)
- Prolonged hypoxia, cell
death & fibrosis of
centrilobular zones
- Biliary Fibrosis
- Chronic periportal
inflammation,
cholangitis/cholangiohepatitis
&/or biliary obstruction
- Usually fibrosis
in portal areas
- Chronic periportal
inflammation,
cholangitis/cholangiohepatitis
&/or biliary obstruction
- Post-necrotic scarring
- Following a single episode of
widespread (massive)
hepatocellular necrosis
- Parenchyma & connective
tissue scaffold (reticulin) are
damaged
- Post-necrotic
collapse
- Affected area cannot
regenerate & is
replaced by fibrous
tissue
- Following a single episode of
widespread (massive)
hepatocellular necrosis
- Diffuse Hepatic
Fibrosis
- On-going (Chronic)
hepatocyte necrosis =>
Overwhelms the
regenerative capacity
- Chronic toxic injury =>
Phenobarbital,
copper-associated, chronic
inflammation
- Widespread
fibrous tissue
deposition
- Deposition of connective tissue
in space of Disse =>Loss of
fenestrations in sinusoidal
endothelium (capillarisation) =>
Reduced permeability =>
Impaired blood-hepatocyte
exchange
- On-going (Chronic)
hepatocyte necrosis =>
Overwhelms the
regenerative capacity
- Localized or generalized
deposition of extracellular
connective tissue matrix
(fibrous/scar tissue) as a healing
response to hepatic injury
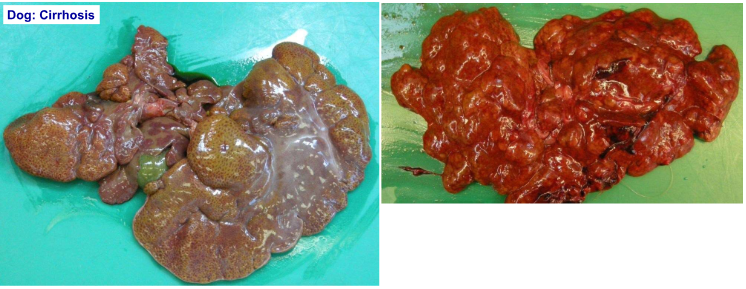
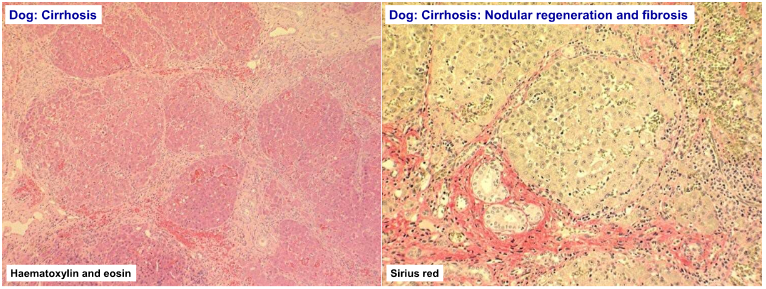
- Cirrhosis
- Diffuse, irreversible,
end-stage hepatic
disease
- Combination
of:
- Hepatocyte
destruction
- Nodular
regeneration
- Biliary
hyperplasia
- Bridging fibrosis (across
portal areas)
- Portal-centrilobular
vascular anastomoses
- Portal-centrilobular
vascular anastomoses
- Bridging fibrosis (across
portal areas)
- Biliary
hyperplasia
- Nodular
regeneration
- Hepatocyte
destruction
- Mostly seen in
Dogs
- Hepatic
insufficiency
- Liver failure
- Cause cannot always
be established
- Cause cannot always
be established
- Liver failure
- Hepatic
insufficiency
- Pathology:
- Hypoproteinaemia:Ascites
- Icterus:
Hyperbilirubinaemia
- Coagulopathy
- Hepatic encephalopathy:
NH3 retention
- 2ndary photosensitisation:
Herbivores (Phylloerythrin
not excreted due to
cholestasis)
- Hypoproteinaemia:Ascites
- Diffuse, irreversible,
end-stage hepatic
disease
- Hypertrophy of Hepatocytes
- Hepatic Mechanical Conditions
(Trauma)
- Displacement
- Aquired
displacement
of Liver
- RTA
- Dogs, Cats
- Liver lobe
torsion
- Liver lobe
torsion
- Dogs, Cats
- Aquired
displacement
of Liver
- Rupture
- Compression
trauma
- RTA (Dogs &
Cats)
- Abuse (Ex. kicks: Dogs &
Cats)
- Overlying (Piglets crushed by
Sow)
- "High rise
syndrome"
(Dogs & Cats)
- "High rise
syndrome"
(Dogs & Cats)
- Overlying (Piglets crushed by
Sow)
- Abuse (Ex. kicks: Dogs &
Cats)
- Compression
trauma
- Displacement
- Developmental
Conditions
- Congenital
Cysts
- Biliary cysts
- Isolated or
clusters
- Formed from bile
ductules
- Concurrent polycystic
kidney disease
- Concurrent polycystic
kidney disease
- Formed from bile
ductules
- Pigs,
Calves,Lambs,
Kittens, Dogs
- Isolated or
clusters
- Biliary cysts
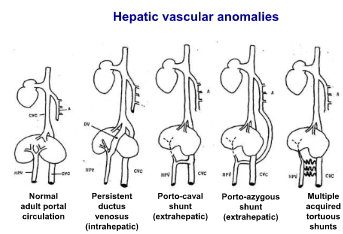
- Congenital vascular
anomalies
- Portosystemic
Shunts
- Anomalous development of
portal vein
- Extrahepatic: Prior to
liver
- Intrahepatic: Within
liver
- Persistent
ductus
venosus
- Persistent
ductus
venosus
- Porto-caval;
Porto-azygous
- Intrahepatic: Within
liver
- Extrahepatic: Prior to
liver
- Sxs (Dogs, Cats):
- Failure to
gain weight,
illthrift
- Hepatic
encephalopathy
- Failure to
gain weight,
illthrift
- Hypoplasia of liver & portal vein
- Histopath:
- Absence of
portal venules
(portal
circulation
diverted
elsewhere)
- Proliferation of
Hepatic
arterioles
- Absence of
portal venules
(portal
circulation
diverted
elsewhere)
- Anomalous development of
portal vein
- Primary portal vein hypoplasia
- Microvascular dysplasia
- Microvascular dysplasia
- Intrahepatic arteriovenous fistulae
- B/w Hepatic artery & portal vein
- B/w Hepatic artery & portal vein
- Portosystemic
Shunts
- Hepatic
Displacement
- Congenital pericardial diaphragmatic
hernia
- Proplapse of one or
more liver lobes into
thorax (pericardial
sec)
- Persian cats
- Persian cats
- Opening in
diaphragm to
pericardial sac
- Proplapse of one or
more liver lobes into
thorax (pericardial
sec)
- Congenital pericardial diaphragmatic
hernia
- Biliary atresia
- Absence of
bile ducts &
ductules
- Absence of
bile ducts &
ductules
- Absence of
gallbladder
- Congenital
Cysts
- Acquired Disturbances of Hepatic
Circulation
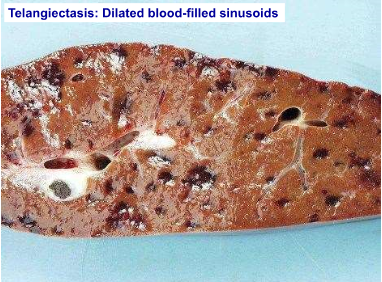
- Telangiectasis
- Dilation (ectasia) of
groups of sinusoids
- Filled w/
blood
- Incidental
finding
- Cattle, Cats
- Cattle, Cats
- Incidental
finding
- Filled w/
blood
- Dilation (ectasia) of
groups of sinusoids
- Vascular
Obstruction
- Portal Vein
- Total rapid
obstruction:
- Death as a result of
hypovolemic shock
(sequestration of blood in
splanchnic bed)
- Medical
Emergency
- Medical
Emergency
- Death as a result of
hypovolemic shock
(sequestration of blood in
splanchnic bed)
- Partial or slowly
progressive
occlusion:
- Atrophy of lobes of liver,
depending on development of
accessory portal circulation
- When accessory
circulation is inadequate,
portal hypotension
develops => Congestion &
ascites
- Aquired porto-systemic vascular
shunting
- Collateral blood vessels
bypass the normal route of
blood flow through the
liver
- Secondary to Portal Hypertension
- Severe hepatic disease
(fibrosis/cirrhosis)
- Occlusion of the
hepatic vein or portal
vein
- Arteriovenous
fistulae
- Primary portal vein
hypoplasia
- Primary portal vein
hypoplasia
- Arteriovenous
fistulae
- Severe hepatic disease
(fibrosis/cirrhosis)
- Secondary to Portal Hypertension
- Dogs & Cats
- Caval obstruction/chronic venous
congestion of HEART FAILURE does
NOT result in acquired shunts (No
pressure gradient, caudal venacava &
hepatic circulation are equally
affected)
- Collateral blood vessels
bypass the normal route of
blood flow through the
liver
- When accessory
circulation is inadequate,
portal hypotension
develops => Congestion &
ascites
- Atrophy of lobes of liver,
depending on development of
accessory portal circulation
- Total rapid
obstruction:
- Portal Vein
- Telangiectasis
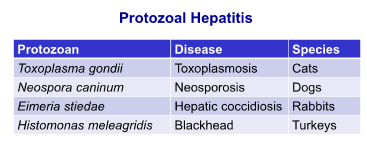
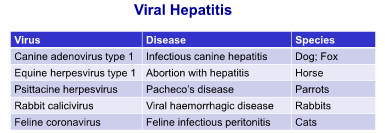
- Hepatitis
- Acute Hepatitis
- Usually associated w/
hepatocellular
necrosis
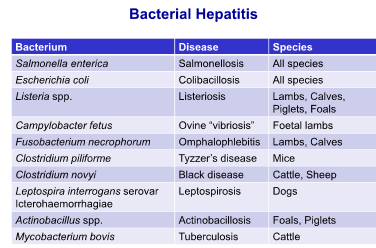
- Suppurative
necrotizing hepatitis
(Bacterial infections)
- Salmonellosis
- Salmonellosis
- Eosinophilic
hepatitis (Parasitic
infections)
- Larval forms migrate
through liver =>
Hepatitis
- Larval forms migrate
through liver =>
Hepatitis
- Suppurative
necrotizing hepatitis
(Bacterial infections)
- Usually associated w/
hepatocellular
necrosis
- Chronic Hepatitis
- Chronic inflammatory
stimulus
- Fibrovascular hyperplasia (Granulation
tissue)
- Nodular
regeneration
- Fibrosis
- Cellular inflammatory
infiltrates
- Lymphocytes & plasma cells (portal
areas)
- Eosinophils (Portal
areas)
- Granulomatous
inflammation
- Lymphocytes & plasma cells (portal
areas)
- Cellular inflammatory
infiltrates
- Fibrosis
- Nodular
regeneration
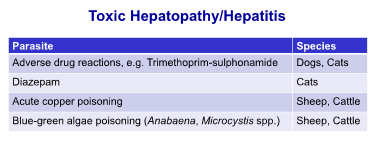
- Copper-associated hepatopathy
(Dogs)
- Chronic copper toxicity
(Sheep)
- Ragwort toxicity (Due to pyrrolizidine
alkaloids) (Horses, Cattle, Sheep)
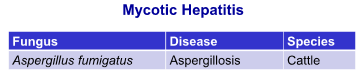
- Alfatoxins (aspergillus flavus)
on stored grain (Pigs, Sheep)
- Ascaris suum
(pigs)
- Milk spot
liver
- Milk spot
liver
- Ascaris suum
(pigs)
- Alfatoxins (aspergillus flavus)
on stored grain (Pigs, Sheep)
- Ragwort toxicity (Due to pyrrolizidine
alkaloids) (Horses, Cattle, Sheep)
- Chronic copper toxicity
(Sheep)
- Chronic venous congestion w/
hepatocyte fatty degeneration &
necrosis
- Chronic inflammatory
stimulus
- Cholangiohepatitis
- Inflammation of the biliary
tree & hepatocellular
parenchyma
- Inflammation starts in the bile
ducts & extends into
parenchyma
- Inflammation starts in the bile
ducts & extends into
parenchyma
- Chronic fascioliasis in
ruminants
- Bacterial cholangiohepatitis from
ascending infections from the
intestine to the bile ducts
- Cats: Chronic
Cholangiohepatitis
- In association w/
chronic
pancreatitis &/or
enteritis
- => Triaditis (possibly due
to common entry of bile &
pancreatic ducts into the
small intestine)
- => Triaditis (possibly due
to common entry of bile &
pancreatic ducts into the
small intestine)
- In association w/
chronic
pancreatitis &/or
enteritis
- Cats: Chronic
Cholangiohepatitis
- Bacterial cholangiohepatitis from
ascending infections from the
intestine to the bile ducts
- Inflammation of the biliary
tree & hepatocellular
parenchyma
- Acute Hepatitis
- Biliary Disease
- Cholangitis
- Affects intra &/or
extra Hepatic bile
ducts
- Usually an
ascending infection
- Chronic lymphocytic cholangitis (Cats)
- Excessive aggregation of
lymphocytes in portal tracts,
bile duct proliferation & portal
fibrosis
- Possibly immune mediated
- Possibly immune mediated
- Excessive aggregation of
lymphocytes in portal tracts,
bile duct proliferation & portal
fibrosis
- Affects intra &/or
extra Hepatic bile
ducts
- Cholecystitis
- Inflammation of the gallbladder
- Acute or Chronic
- Ascending infection:
Salmonella enterica
- Inflammation of the gallbladder
- Cystic mucinous hyperplasia
- Hyperplasia of
the gallbladder &
lining epithelium
- Abundant production of mucous
- Severe distension (mucocoele)
- Obstruction (RARE)
- Severe distension (mucocoele)
- Hyperplasia of
the gallbladder &
lining epithelium
- Stenosis of the bile duct
- External compression
- Fibrosis, Inflammation, Tumors
- Fibrosis, Inflammation, Tumors
- External compression
- Cholelithiasis
- Gall stones (Choleliths)
- Usually form in
gallbladder
- Mixture: Bilirubin, Ca carbonate,
glycoprotein
- Mixture: Bilirubin, Ca carbonate,
glycoprotein
- Usually form in
gallbladder
- Dogs, Cats
- Cattle (Incidental
finding)
- Complete obstruction =>
Extrahepatic cholestasis =>
Jaundice
- Leakage of bile into portal
areas => inflammation &
fibrosis
- Gall stones (Choleliths)
- Cholangitis
- Hepatic
Neoplasia
- Hepatocellular carcinomas
are more common than
hepatocellular adenomas
- Cholangiocarcinomas &
Cholangioadenomas - Tumors
of the gallbladder
(Uncommon)
- Vascular tumors -
Haemangiosarcoma
- Metastatic neoplasia (To
Liver)
- Ex. Pancreatic carcinoma,
intestinal adenocarcinoma,
splenic haemangiosarcoma
- Ex. Pancreatic carcinoma,
intestinal adenocarcinoma,
splenic haemangiosarcoma
- Multicentric
neoplasia
- Lymphoma or
leukaemia
- Lymphoma or
leukaemia
- Hepatocellular carcinomas
are more common than
hepatocellular adenomas
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.