374250
Beschreibung
Mindmap von melian.yates, aktualisiert more than 1 year ago
|
|
Erstellt von melian.yates
vor etwa 11 Jahre
|
|
Respiratory Pathology
- Routes of Invasion
- 1) Aerogenous
- Trachea: High speed
- Bronchi/bronchioles:
Slower speed
- => Aerogenous particles
settle (Cranioventral areas)
- => Aerogenous particles
settle (Cranioventral areas)
- Bronchi/bronchioles:
Slower speed
- Cranial & Medial lobes
- Trachea: High speed
- 2) Haemotogenous
- Random scattering of
multifocal lesions
- Ex. Metastases
- Ex. Metastases
- Random scattering of
multifocal lesions
- 3) Transcoelomic
- Ex. Traumatic Reticulitis
(Entry through Diaphragm)
- Ex. Traumatic Reticulitis
(Entry through Diaphragm)
- 1) Aerogenous
- Nasal Cavity
- Normal flora:
- Variable (Gram +ve)
- Prevent adherence
by pathogenic (often
Gram -ve bacteria)
- Prevent adherence
by pathogenic (often
Gram -ve bacteria)
- Variable (Gram +ve)
- Circulatory Problems
- Epistaxis
- Ex. Equine Ethmoid
Haematoma
- Chronic nasal bleeding
- Old horses
- Pedunculated mass in
ethmoidal region
- Expansive, but
non-neoplastic
- Progressive Ethmoid
Haematoma (PEH)
- Gets bigger over time
- Gets bigger over time
- Progressive Ethmoid
Haematoma (PEH)
- Expansive, but
non-neoplastic
- Pedunculated mass in
ethmoidal region
- Old horses
- Chronic nasal bleeding
- Epistaxis
- Rhinitis
- Infectious (Upper
Resp. tract infections)
- Viruses
- Bacteria
- Fungi
- Ex. Aspergillus
fumigatus
- Chronic necrotizing
inflammation => destruction
of turbinates & septum
- Chronic necrotizing
inflammation => destruction
of turbinates & septum
- Cryptococcus neoformans
- Nasal cavity
often affected
- Sneezing, nasal
discharge, nasal swelling
(Granulomatous rhinitis)
- +/- Skin, ocular &
CNS lesions
- +/- Skin, ocular &
CNS lesions
- Sneezing, nasal
discharge, nasal swelling
(Granulomatous rhinitis)
- Has a thick,
non-staining
mucoid capsule
- Nasal cavity
often affected
- Ex. Aspergillus
fumigatus
- Ex. Atrophic rhinitis
- Strangles (Streptococcus equi)
- Lymphadentitis, Pharyngitis, Rhinitis,
Metastatic abcesses, Guttural pouch
empyema, Purpura haemorrhagica
- Lymphadentitis, Pharyngitis, Rhinitis,
Metastatic abcesses, Guttural pouch
empyema, Purpura haemorrhagica
- Fungi
- Ex. Feline viral rhinotracheitis,
Canine distemper, Infectious
Bovine Rhinotracheitis, Equine
Rhinovirus
- Bacteria
- Viruses
- Allergens
- Toxins
- Trauma/foreign
bodies
- Classification
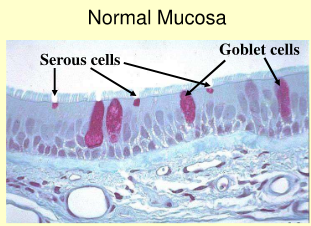
- Serous
- Catharral
- Mucopurulent
- Purulent
- Fibrinous
- Ulcerative
- + Fibrinonecrotic =>
Full thickness of
epithelium exposed
- + Fibrinonecrotic =>
Full thickness of
epithelium exposed
- Fibrin deposits
- Ulcerative
- Fibrinous
- Overproduction of Mucous
(Goblet cells) + Neutrophil
Infiltration => Snotty nose
- Purulent
- Overproduction of
mucous by Goblet cells
- Mucopurulent
- Overproduction of Serous
fluid (by Serous cells)
- Catharral
- Serous
- Chronic Rhinitis
- Consequence of Acute
Rhinitis failing to resolve
- Chronic purulent rhinitis
- Nasal Polyps
- Consequence of Acute
Rhinitis failing to resolve
- Allergic Rhinitis
- Hypersensitivity to
inhaled allergens
- Nasal epithelium damaged
by cytokines
- Succeptible to 2ndary
bacterial infections
- Eosinophils often the
dominant infiltrating
leukocyte
- Eosinophils often the
dominant infiltrating
leukocyte
- Succeptible to 2ndary
bacterial infections
- Hypersensitivity to
inhaled allergens
- Infectious (Upper
Resp. tract infections)
- Pseudostratified columnar epithelium
- Sinusitis
- Common
sequel to
Rhinitis
- Close proximity of
sinuses to nasal
cavity (Blockage of
sinus drainage)
- Purulent inflammation of the
sinuses -> Chronic (poor
drainage)
- Dental or peridontal
disease (maxillary
sinus)
- Penetration of infections
from dehorning wounds &
fractures of the facial bones
(Frontal sinus)
- Penetration of infections
from dehorning wounds &
fractures of the facial bones
(Frontal sinus)
- Common
sequel to
Rhinitis
- Neoplasia (Nasal Cavity & Sinuses)
- Generally rare (more
common in Dogs)
- Can arise from any of
the tissues in the region
- Adenoma/carcinoma
(Glands/epthelium)
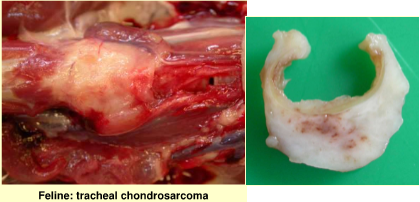
- Sarcoma (Cartilage,
bone, connective tissue)
- Sarcoma (Cartilage,
bone, connective tissue)
- Adenoma/carcinoma
(Glands/epthelium)
- Most are malignant
& are usually 2ndarily
infected
- Ex. Endemic ethmoid tumors
(Ruminants): Retroviral origin -
Carcinomas
- Generally rare (more
common in Dogs)
- Normal flora:
- Conducting Airways
- Larynx & Trachea
- Airflow obstruction
- Aspiration pneumonia
- Necrotic Laryngitis
- Ex. Calves: Fusobacterium
necrophorum
- Friable appearance
- Friable appearance
- Cranial /Ventral lung lobes
- Massive
inflammatory rxn
(rupture onto surface)
- Massive
inflammatory rxn
(rupture onto surface)
- Ex. Calves: Fusobacterium
necrophorum
- Laryngeal Chondritis
- Texels & Southdowns
(Other breeds)
- Rams > Ewes
- Chronic suppuration w/in the
arytenoid cartilages of the larynx
resulting in swelling & occlusion of the
lumen (of larynx)
- Texels & Southdowns
(Other breeds)
- Filaroides Osleri
- Parasite (Canine)
- Nodules around
tracheal bifurcation
- Foreign body nodular
rxn develops around
dead parasites
- Parasite (Canine)
- Tracheitis
- Thickening, hyperplasia
of lamina propria
- 2ndary bacterial infections
- Clumps of necrotizing debris
- Clumps of necrotizing debris
- 2ndary bacterial infections
- Runny nose,
runny eyes
- High
morbidity,
low mortality
- Ex. Infectious Bovine Rhinotracheitis
- Thickening, hyperplasia
of lamina propria
- Non-inflammatory Tracheal Diseases
- Tracheal Collapse
- Dorsoventral
tracheal flattening
- Tracheal ligament
has become
stretched
- Older, small breed dogs
- Older, small breed dogs
- Tracheal ligament
has become
stretched
- Dorsoventral
tracheal flattening
- Tracheal Neoplasia (Uncommon)
- Tracheal Collapse
- Airflow obstruction
- Bronchi
- Bronchitis
- Acute
- Chronic
- Goblet cell hyperplasia
& hypersecretion
- Squamous metaplasia
- Bronchiectasis
- Permanent dilation
of bronchi (as a result
of accumulation of purulent
exudate in the lumen)
- Partial rupture of
bronchial walls
(irreversible)
- Usually 2ndary to
chronic bronchitis
- Grape bunch appearance
- Permanent dilation
of bronchi (as a result
of accumulation of purulent
exudate in the lumen)
- Bronchiectasis
- Squamous metaplasia
- Dogs:
- Chronic cough
- Excess airway exudate
- Thickened mucosa
- Chronic inflammation
- => Stimulation of muscular
hypertrophy in walls of
small arteries
- Pulmonary hypertension
=> Cor pulmonale (RT
heart failure)
- Pulmonary hypertension
=> Cor pulmonale (RT
heart failure)
- => Stimulation of muscular
hypertrophy in walls of
small arteries
- Chronic inflammation
- Thickened mucosa
- Excess airway exudate
- Chronic cough
- Goblet cell hyperplasia
& hypersecretion
- Acute
- Infectious tracheobronchitis
(Kennel Cough)
- Common
- Persistent
tracheobronchial
inflammation
- If severe => Rhinitis or
Bronchopneumonia
- If severe => Rhinitis or
Bronchopneumonia
- Bordetella bronchiseptica
- PI2
- CAV2
- CAV2
- PI2
- Common
- Bronchioles
- Epithelium highly
susceptible to
injury:
- Presence of Clara cells
(contain oxidases that
can locally generate
metabolites that are
toxic)
- Vulnerability
to free radical
damage
- Vulnerability
to free radical
damage
- Presence of Clara cells
(contain oxidases that
can locally generate
metabolites that are
toxic)
- Bronchiolitis
- Bronchiolar Obstruction
- Bronchioles much more
prone to obstruct when
inflamed than Bronchi
- Not much cartilage
(rigid structure) ->
Fills w/ inflammatory
cells
- Where collateral ventilation is
poor (Ruminants) obstructed
bronchiole -> Atelectasis
- Not much cartilage
(rigid structure) ->
Fills w/ inflammatory
cells
- Bronchioles much more
prone to obstruct when
inflamed than Bronchi
- Extension of or concurrently
w/ Bronchitis & Pneumonia
- Certain viral infections
(pulmonary toxicity)
- When exudate cannot be cleared ->
infiltration by fibroblasts ->
development of organized polyp-like
masses w/in the bronchiolar lumen
=> Bronchiolitis Obliterans
- Bronchiolar Obstruction
- Epithelium highly
susceptible to
injury:
- Bronchitis
- Larynx & Trachea
- Alveoli
- Structure
- Simple squamous epithelium
- Type 1 Pneumocytes: Flattened, fried
egg, cover 97% of septal surface
- Type 2 Pneumocytes: Cuboidal,
cover approx. 3% of septal surface
- Produce Surfactant
- Progenitor of Type I &
Type II Pneumocytes
- Repair surface of lungs
(Damage)
- Repair surface of lungs
(Damage)
- Produce Surfactant
- Type 1 Pneumocytes: Flattened, fried
egg, cover 97% of septal surface
- Simple squamous epithelium
- Response to Injury
- Aveolar Epithelialisation
- Marked lung damage (Type II
Pneumocytes predominate)
- Marked lung damage (Type II
Pneumocytes predominate)
- Hyaline Membrane Formation
- Severe & Acute
lung disease
- Stain pink
- Severe & Acute
lung disease
- Aveolar Epithelialisation
- Pneumonia
- Consolidation = altered texture of
lung (firmer) due to accumulation of
exudates (fluid & cellular infiltrate)
- Inflammation that takes
places in the alveoli &
their walls
- Classification via:
- Nature of inflammatory process
- Aetiological agent
- Pattern
- Pattern
- Aetiological agent
- Nature of inflammatory process
- Bronchopneumonia
- From terminal bronchioles
- Aerogenous portal of
entry => Cranioventral
- Aerogenous portal of
entry => Cranioventral
- Common (Bacterial, Mycoplasmal)
- Neutrophils & cell debris =>
- Sequella:
- Resolution (mucociliary
escalator, resolves 3 -4 weeks)
- Progression => Chronic
Suppurative
Bronopneumonia
- Consequences:
- Bronchiectasis
- Pulmonary abcessation
- Pleuritis & adhesions
- Atelectasis or overinflation
- BALT hyperplasia
- BALT hyperplasia
- Atelectasis or overinflation
- Pleuritis & adhesions
- Pulmonary abcessation
- Bronchiectasis
- Consequences:
- Resolution (mucociliary
escalator, resolves 3 -4 weeks)
- Sequella:
- Fibrinous Bronchopneumonia
- Acute (tends to be more
severe than suppurative)
- => Sudden death (possible) -
toxaemia (Pasteurella)
- => Fibrosis &
adhesions (b/w
visceral & parietal
pleura)
- Acute (tends to be more
severe than suppurative)
- Bronchointerstitial Pneumonia
- Hybrid of Bronchopneumonia
& Interstitial Pneumonia
- Caused by viruses damaging
both airway & alveolar
epithelial cells (Ex. RSV)
- Hybrid of Bronchopneumonia
& Interstitial Pneumonia
- From terminal bronchioles
- Interstitial Pneumonia
- Inflammation primarily
in alveolar walls
- Haematogenous
spread (Most cases)
- Diffuse damage
- Diffuse damage
- (May)=> Protein & fluid
exudation => Hyaline
membrane formation
- Exudative phase followed by
proliferative phase (Type II
pneumocytes proliferate to
replace damaged Type I cells)
- Acute
- May be transient
(Ex. viral infections)
- May be severe & associated
with life threatening pulmonary
oedema (Ex. Acute Resp.
distress syndrome -ARDS)
- Examples:
- Fog Fever (Acute
Bovine Pulmonary
Oedema & Emphysema)
- Adult beef cattle
- Autumn (change to lush pasture)
- Ingestion of Tryptophan
(3 methyl indole) in rumen
- Local generation of Free
Radicals => Necrosis of
Type I Pneumocytes
- Hyaline formation => Acute
interstitial Pneumonia =>
Chronic Interstitial Pneumonia
- Hyaline formation => Acute
interstitial Pneumonia =>
Chronic Interstitial Pneumonia
- Local generation of Free
Radicals => Necrosis of
Type I Pneumocytes
- Ingestion of Tryptophan
(3 methyl indole) in rumen
- Autumn (change to lush pasture)
- Adult beef cattle
- Paraquat Poisoning
- Weed killer
(uncommon)
- Dogs & Cats
- Acute & Chronic lesions
- Extrapulmonary lesions
- Necrosis of adrenal
zona glomerulosa
- Necrosis of Renal tubular
epithelium
- Necrosis of Renal tubular
epithelium
- Necrosis of adrenal
zona glomerulosa
- Weed killer
(uncommon)
- Fog Fever (Acute
Bovine Pulmonary
Oedema & Emphysema)
- May be transient
(Ex. viral infections)
- Chronic
- Dominated by fibrosis of
alveolar walls &
proliferation of Type II
Pneumocytes
- Dominated by fibrosis of
alveolar walls &
proliferation of Type II
Pneumocytes
- Inflammation primarily
in alveolar walls
- Embolic Pneumonia
- Haematogenous spread
- Most often Caudal (Can
occur anywhere)
- B/c more lung tissue
- B/c more lung tissue
- Oriented around blood
vessels (Embolis must
come in vascular supply)
- Haematogenous spread
- Granulomatous Pneumonia
- Dominated by
macrophages, +/-
giant cells
- Varying associated
lymphocytes &
neutrophils
- Multiple granulomas
scattered throughout
the lungs
- Dominated by
macrophages, +/-
giant cells
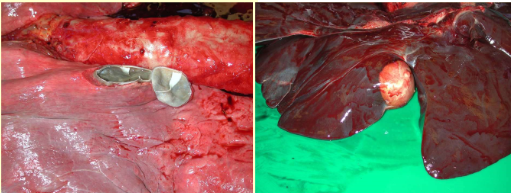
- Pulmonary Abscesses
- 1) Extension from Pneumonia
- 2) Septic emboli
- Ex. Suppurative mastitis
- Ex. Suppurative mastitis
- 3) Aspiration of foreign material
- 4) Direct penetration
- Ex. Traumatic
reticulocarditis
- Ex. Traumatic
reticulocarditis
- 1) Extension from Pneumonia
- Enzootic Pneumonia
- Young animals in close contact
(Calves, Lambs & Pigs)
- Young animals in close contact
(Calves, Lambs & Pigs)
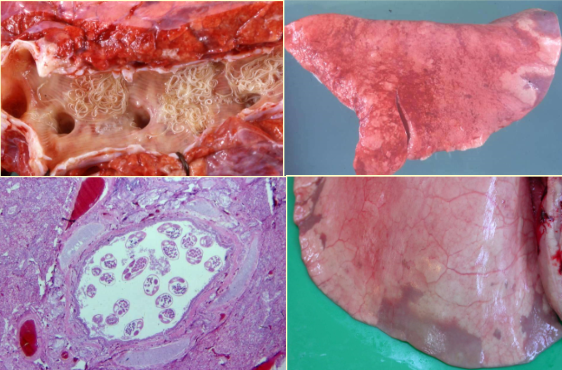
- Parasitic Disease
- Dictyocaulus viviparus
- Lifecycle
- Penetration phase
- In transit
- In transit
- Prepatent phase
- Sequential alveolitis ->
bronchiolitis -> bronchitis
- Sequential alveolitis ->
bronchiolitis -> bronchitis
- Patent Phase
- Parasitic bronchitis & pneumonia
- Parasitic bronchitis & pneumonia
- Postpatent Phase recovery
- Acute signs due to:
- Alveolar epithelialisation
- Superimposed infection
- Superimposed infection
- Alveolar epithelialisation
- Acute signs due to:
- Penetration phase
- Wedge-shaped lesions
- Lifecycle
- Dictyocaulus filaira
- Dictyocaulus arnfeldi
- Common (rarely
clinical disease)
- Horses & Donkeys
- Gross pathology
- Raised focal
over-inflated areas in
the caudal lung lobes
- Raised focal
over-inflated areas in
the caudal lung lobes
- Histology
- Central parasites &
associated chronic
catharral bronchitis
- Hyperplastic bronchial
epithelium & surrounding
lymphoid infiltration
- Central parasites &
associated chronic
catharral bronchitis
- Common (rarely
clinical disease)
- Metastrongylus (Pigs)
- Muellerius capillaris
- Common (rarely
clinical sig.)
- Firm "lead shot" nodules
- Dorsal regions of caudal lobes
- Common (rarely
clinical sig.)
- Aerostrongylus abstrusus
- Cat lungworm
- Firm, yellow nodules
in parenchyma
- Eggs & larvae ->
Foreign body type
Rxn
- Chronic coughing & airway
Eosinophilia (can resemble
asthma)
- Cat lungworm
- Angiostrongylus vasorum (Heart worm)
- Pulmonary arteries &
RT ventricle
- Dogs & Foxes
- Can cause proliferative change in
blood vessels => Pneumonia =>
Pulmonary Oedema & Hypertension
- Pulmonary arteries &
RT ventricle
- Echinococcus granulosus
- Intermediate stage (Lungs)
- Little clinical significance
- Zoonosis & carcass
condemnation
- Hydatid Cyst
- Hydatid Cyst
- Zoonosis & carcass
condemnation
- Intermediate stage (Lungs)
- Hypersensitivity Diseases
- Type I Hypersensitivity
- Mast cell mediated
(Through Ag- IgE
complexes)
- => Degranulation
- Constriction of airways
- Constriction of airways
- => Degranulation
- Feline Asthma/
Allergic Bronchitis
- Inhaled Ags
- Recurrent episodes
of bronchoconstriction
- Inflammation
(Eosinophil dominated)
- +/- Circulating Eosinophilia
- +/- Circulating Eosinophilia
- Inflammation
(Eosinophil dominated)
- Inhaled Ags
- Pulmonary
Infiltration w/
Eosinophilia
- Dog
- Predominance of
Eosinophils in airways
- Inhaled Ags
- Dog
- Mast cell mediated
(Through Ag- IgE
complexes)
- Type III Hypersensitivity
- Ag-Ab Complex mediated
- Can settle in
alveolar blood
vessels
- Can settle in
alveolar blood
vessels
- Extrinsic Allergic
Bronchio-alveolitis
- Repeat inhalation of spores
- Chronic inflammation
- Thickening of alveolar septae
- Thickening of alveolar septae
- Chronic inflammation
- Housed Dairy Cows (Winter)
- Diffuse Fibrosing Alveolitis (DFA)
- Repeat inhalation of spores
- COPD - Chronic Obstructive
Pulmonary Disease (SPAOPD
-Summer pasture associated)
- Chronic coughing,
poor performance
- Airway inflammation, excess mucus
- Airway inflammation, excess mucus
- Heaves (Heave line)
- Gross:
- Affected lungs
unremarkable (except in
extreme cases - alveolar
emphysema)
- Affected lungs
unremarkable (except in
extreme cases - alveolar
emphysema)
- Histologically:
- Chronic generalized bronchitis
- Plugging of airways w/ mucous,
inflammatory cells, goblet cell metaplasia &
smooth muscle hypertrophy
- Plugging of airways w/ mucous,
inflammatory cells, goblet cell metaplasia &
smooth muscle hypertrophy
- Chronic generalized bronchitis
- Chronic coughing,
poor performance
- Ag-Ab Complex mediated
- Type I Hypersensitivity
- Dictyocaulus viviparus
- Aspiration Pneumonia
- Inhaling foreign
particle
- Severity depends on nature
of material (ex. food),
bacterial load, & distribution
w/in lungs
- Can develop into
Severe Necrotizing
pneumonia =>
Gangrenous
pneumonia
- Abscesses
- Abscesses
- Inhaling foreign
particle
- Gangrenous Pneumonia
- Tissue becomes necrotic ->
invaded by putrefactive
saphrophytes (Ex. Clostrdia)
- Dead tissue undergoes
Liquefactive Necrosis
- Dead tissue undergoes
Liquefactive Necrosis
- Usually Iatrogenic or
as a sequel to
aspiration pneumonia
- Tissue becomes necrotic ->
invaded by putrefactive
saphrophytes (Ex. Clostrdia)
- Lipid Pneumonia
- Endogenous
- Cats > Dogs
- Subclinical
- Accumulation of lipids
(surfactant) in pulmonary
macrophages -> multifocal
white nodules
- Cats > Dogs
- Exogenous
- Associated w/
inhalation of oil,
paraffin, etc.
- Rxn dominated by
macrophages which fill
the alveoli
- Interstitial thickening
(mononuclear cells &
fibrosis) - Inflammation
- Associated w/
inhalation of oil,
paraffin, etc.
- Endogenous
- Uraemic Pneumonia
- Sever uraemia =>
increased permeability
of the blood -air barrier
- (May) => Pulmonary Oedema
- (May) => Degeneration &
calcification of smooth
muscle & connective tissue
- Sever uraemia =>
increased permeability
of the blood -air barrier
- Consolidation = altered texture of
lung (firmer) due to accumulation of
exudates (fluid & cellular infiltrate)
- Structure
- Pulmonary Oedema
- Protection Mechanisms
- Impermeable epithelium & junctions
- Interstitial pressure in
alveolar septae lower than
intraalveolar pressure
- Efficient lymphatic drainage
- Pushes fluid out
of alveoli
- Efficient lymphatic drainage
- Interstitial pressure in
alveolar septae lower than
intraalveolar pressure
- Impermeable epithelium & junctions
- Excessive fluid in the lung
- Begins as Interstitial Oedema
- Expansion of perivascular,
peribronchial & peribronchiolar fascia
& distension of interstitial lymphatics
- Interstitial compartment overwhemled =>
fluid floods airspces => Alveolar oedema
- Expansion of perivascular,
peribronchial & peribronchiolar fascia
& distension of interstitial lymphatics
- Causes
- Increased capillary or Type I
epithelial permeability
- Systemic toxins
- Shock
- Inhaled caustic gases
- Systemic toxins
- Increased capillary hydrostatic
pressure (cardiogenic oedema)
- LT sided or
Biventricular
Heart failure
- Increased hydrostatic
pressure -> pushes fluid into
lungs
- LT sided or
Biventricular
Heart failure
- Decreased plasma oncotic
pressure (Hypoalbuminaemia)
- Proteins keep fluid in
plasma (Decreased proteins
-> fluid leaves vascular
compartment -> Lungs)
- Proteins keep fluid in
plasma (Decreased proteins
-> fluid leaves vascular
compartment -> Lungs)
- Increased capillary or Type I
epithelial permeability
- Protection Mechanisms
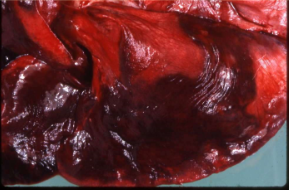
- Pulmonary Haemorrhage
- Embolism, Thrombosis & Infarction
- Lung supplied by BOTH Pulmonary
& Bronchial Arteries
- Infarction doen NOT usually
follow embolism or
thrombosis, UNLESS
pulmonary circulation is
already compromised
- Usually occur w/
emboli/thrombosis during general
circulatory collapse or passive
congestion of heart failure
- Usually occur w/
emboli/thrombosis during general
circulatory collapse or passive
congestion of heart failure
- Infarction doen NOT usually
follow embolism or
thrombosis, UNLESS
pulmonary circulation is
already compromised
- Lung supplied by BOTH Pulmonary
& Bronchial Arteries
- Pulmonary Hypertension
- Caused by LT -> RT
vascular shunts or Increased
resistance of the pulmonary
vascular system
- Most commonly a sequel of:
- Widespread fibrosis in the lung
- Chronic bronchitis or
bronchiolitis (stimulates
hypertrophy in the walls of
small arteries)
- Chronic bronchitis or
bronchiolitis (stimulates
hypertrophy in the walls of
small arteries)
- Widespread fibrosis in the lung
- Severe, Prolonged =>
Cor Pulmonale
- RT-sided Heart failure
2ndary to primary lung
disease
- RT-sided Heart failure
2ndary to primary lung
disease
- Caused by LT -> RT
vascular shunts or Increased
resistance of the pulmonary
vascular system
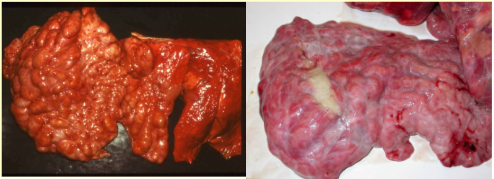
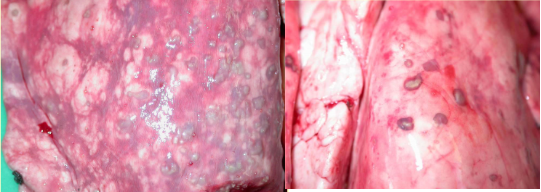
- Neoplasia
- Pulmonary Tumors
- Metastatic: Common
- OPA (Ovine Pulmonary Carcinoma)/
Jaagsiekte
- Retrovirus induced cancer
- Intensive management
systems - Aerosol
transmission
- 'Wheelbarrow test'
- Well differentiated carcinoma
- Can get dry forms of
OPA (cells not so active
in producing surfactant)
- Retrovirus induced cancer
- OPA (Ovine Pulmonary Carcinoma)/
Jaagsiekte
- Primary: Relatively Rare
- Dogs & Cats
- Dogs & Cats
- Metastatic: Common
- Bronchial papilloma
- Bronchial adenoma/carcinoma
- Arising from major airways
- Arising from major airways
- Bronchioloalveolar adenoma/carcinoma
- Arising from small airways or alveolar
parenchyma (either secretory
bronchiolar cells or Type II epithelial
cells)
- Carcinoid
- Neuroendocrine cells (Rare in animals)
- Neuroendocrine cells (Rare in animals)
- Arising from small airways or alveolar
parenchyma (either secretory
bronchiolar cells or Type II epithelial
cells)
- Mesothelioma
- Most common in
Calves (can be
congenital)
- Often causes Thoracic effusion
- Multiple nodular masses
on pleural surface &
visceral surface
- Dx can be difficult due to
cytological similarity of reactive &
neoplastic mesothelial cells
- Most common in
Calves (can be
congenital)
- Pulmonary Tumors
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.