395888
Beschreibung
Mindmap von melian.yates, aktualisiert more than 1 year ago
|
|
Erstellt von melian.yates
vor etwa 11 Jahre
|
|
Musculoskeletal Pathology
- Skeletal Muscle
- Muscles of posture,
movement & respiration
- Response of Muscle to Injury
- Degeneration/ Necrosis
- Tends to be
segmental
- (Necrosis of entire myofibre is
uncommon => crush injury or
widespread ischaemia resulting from
pressure on a large artery)
- (Necrosis of entire myofibre is
uncommon => crush injury or
widespread ischaemia resulting from
pressure on a large artery)
- Lots of causes
- Common triggering factor is
increase in Ca2+ w/in the cell
- Allows muscle contraction
- Ca-dependent enzymes &
lysosomal enzymes increase =>
myofibre destruction
- Ca-dependent enzymes &
lysosomal enzymes increase =>
myofibre destruction
- Allows muscle contraction
- Muscle cell contents may leak
into blood if the cell
membrane is damaged
- Creatine kinase (CK) is an enzyme
which leaks following injury & is
commonly used to measure the
extent of muscle damage
- Creatine kinase (CK) is an enzyme
which leaks following injury & is
commonly used to measure the
extent of muscle damage
- Tends to be
segmental
- Regeneration
- Requirements:
- Intact basal lamina (Sarcolemmal tube)
- Blood supply => macrophages
to clear up debris
- Viable satellite cells (act as progenitor
cells for new sarcoplasm production)
- Viable satellite cells (act as progenitor
cells for new sarcoplasm production)
- Blood supply => macrophages
to clear up debris
- If not met,
fibrosis will
occur
- Intact basal lamina (Sarcolemmal tube)
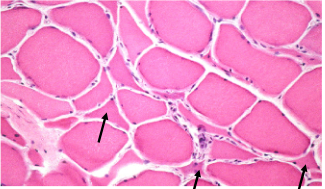
- Skeletal muscle myofibres
have substantial
regenerative ability
- Requirements:
- Atrophy
- Entire muscle or individual
myofibres within are reduced in
diameter
- Causes:
- Disuse (Ex. fracture, failure to
use limb, recumbancy)
- Cachexia, old age, malnutrition
- Denervation (nerve provides
trophic factors: any interference
or damage => muscle atrophy)
- Endocrine disease
- Ex. Equine "roarers" - Laryngeal
hemiplegia (Damage to left
recurrent laryngeal nerve)
- Can be rapid - over
50% of muscle mass lost
in a few weeks
- Endocrine disease
- Denervation (nerve provides
trophic factors: any interference
or damage => muscle atrophy)
- Cachexia, old age, malnutrition
- Disuse (Ex. fracture, failure to
use limb, recumbancy)
- Entire muscle or individual
myofibres within are reduced in
diameter
- Hypertrophy
- Entire muscle or
individual myofibre
diameter increases in
size
- Causes:
- Increased work load
- Compensatory
- Ex. COPD
heaves lines
- Ex. COPD
heaves lines
- Physiological
- Compensatory
- Increased work load
- Entire muscle or
individual myofibre
diameter increases in
size
- Innumerable factors can induce these changes
(Trauma, toxins, infectious agents, nutritional
deficiencies, Ischaemia, Hereditary disease)
- => Specific Dx is NOT POSSSIBLE
based on morphological or histological
features alone
- => Specific Dx is NOT POSSSIBLE
based on morphological or histological
features alone
- Degeneration/ Necrosis
- Muscle Diseases
- Inflammation: Myositis
- Infectious
- Bacteria
- Gain entry via direct penetration,
haematogenously or extension
(Ex. from an infected joint)
- Disease or manifestation
- Abscesses
- Arcanobacterium pyogenes (Bovine, Pigs)
- Streptococcus equi (Equine)
- Corynebacterium pseudotuberculosis
(Sheep, Goats, Equine)
- Arcanobacterium pyogenes (Bovine, Pigs)
- Black leg
- Clostridium chauvoei ( Bovine, Sheep)
- Activation of
latent spores
- Clostridium chauvoei ( Bovine, Sheep)
- Gas gangrene
- Clostridium septicum & C. novyi (Sheep, Bovine,
Equine), C. perfringens & C. sordelli (Pigs)
- Penetrating wounds
- Clostridium septicum & C. novyi (Sheep, Bovine,
Equine), C. perfringens & C. sordelli (Pigs)
- Wooden tongue
- Actinobacillus lignieresii (Bovine)
- Actinobacillus lignieresii (Bovine)
- Abscesses
- Gain entry via direct penetration,
haematogenously or extension
(Ex. from an infected joint)
- Viruses (Rare)
- Parasites
- Nematodes
- Trichinella, Ancylostoma
& Ascarid larvae
- Cestodes
- Taenia solium (cysticercosis
in swine & humans). T.ovis
(cystercercosis in sheep)
- Protozoa
- Toxoplasma gondii,
Neospora caninum,
Sarcocystis
- Toxoplasma gondii,
Neospora caninum,
Sarcocystis
- Taenia solium (cysticercosis
in swine & humans). T.ovis
(cystercercosis in sheep)
- Trichinella, Ancylostoma
& Ascarid larvae
- Nematodes
- Bacteria
- Immune mediated
- Canine Masticatory Muscle Myositis (MMM)
- Autoantibodies SELECTIVELY attack
muscle of mastication (Type IIM fibres)
- Manifests in the masseter &
temporalis muscles (Bilateral)
- Acute stage: Eosinophillic myositis
- Chronic stage: Atrophic myositis
- Chronic stage: Atrophic myositis
- Acute stage: Eosinophillic myositis
- Manifests in the masseter &
temporalis muscles (Bilateral)
- Autoantibodies SELECTIVELY attack
muscle of mastication (Type IIM fibres)
- Extraocular myositis
- Autoantibodies selectively target only
the muscles around the eye in the Dog
- Autoantibodies selectively target only
the muscles around the eye in the Dog
- Canine Polymyositis
- Can affect masticatory muscles but
Dogs DO NOT have antibodies to
type IIM fibres
- Generalized
inflammatory
myopathy
- Muscle necrosis, regeneration & fibrosis
- Muscle enzymes may be increased
- Fever, pain, weakness, resp. distress
- T Lymphocytes, plasma cells, granulocytes
- T Lymphocytes, plasma cells, granulocytes
- Fever, pain, weakness, resp. distress
- Muscle enzymes may be increased
- Single biopsy may not be enough to
make the Dx (it tends to be multifocal
& disseminated)
- DDx = Toxoplasma gondii, MMM
- Can affect masticatory muscles but
Dogs DO NOT have antibodies to
type IIM fibres
- Canine Masticatory Muscle Myositis (MMM)
- Other
- Paraneoplastic,
drug-induced, idiopathic
- Paraneoplastic,
drug-induced, idiopathic
- Infectious
- Congenital
- Defects in muscular form
- Congenital diaphramatic defects
- Myofibrillar hypoplasia
(Pigs - splayleg)
- Can spontaneously
resolve, cause unknown,
responsible for
significant deaths
- Hyperplasia of muscle
fibres (Calves, lambs)
- Double muscling due to
increased number of myofibres
in affected muscle (thighs, rump,
loin) -> Predisposes to dystocia
- Double muscling due to
increased number of myofibres
in affected muscle (thighs, rump,
loin) -> Predisposes to dystocia
- Can spontaneously
resolve, cause unknown,
responsible for
significant deaths
- Myofibrillar hypoplasia
(Pigs - splayleg)
- Congenital diaphramatic defects
- Muscular Dystrophies
- Inherited group (X-linked) of degenerative
muscular diseases causing progressive
muscle weakness & wasting
- Usually due to a genetic fault
leading to a muscular protein
deficiency
- Ex. Duchenne MD in humans
due to dystrophin deficiency
- Dystrophin gene mutations
reported in the Golden
retriever, Rottweiler, Irish
terrier, etc.
- Ex. Duchenne MD in humans
due to dystrophin deficiency
- Innervation is normal
- Muscle biopsy -> confirm lack
of dystrophin with IHC
- Muscle biopsy -> confirm lack
of dystrophin with IHC
- Inherited group (X-linked) of degenerative
muscular diseases causing progressive
muscle weakness & wasting
- Defects in muscular form
- Toxic, Nutritional &
Exertional Myopathies
- Toxic
- Plants
- Gossypol,
Cassia (coffee
senna)
- Gossypol,
Cassia (coffee
senna)
- Drugs
- Monensin
- Coccidiostat
- Toxic to: Horses,
Sheep, Cattle, Dogs,
Birds
- Skeletal & myocardial necrosis
- Rapid onset recumbancy &
potentially death
- Usually due to mixing errors in feed
- Ionophore
- Disturbs transport of
Na & K across
membrane
- Increases Ca2+ =>
Hypercontraction &
Degeneration
- Increases Ca2+ =>
Hypercontraction &
Degeneration
- Disturbs transport of
Na & K across
membrane
- Coccidiostat
- Monensin
- Chemicals
- Ex. Fe injections can
cause local
myonecrosis
- Ex. Fe injections can
cause local
myonecrosis
- Mycotoxins
- Plants
- Endocrine
- Hyperadrenocorticism &
Hypothyroidism => Muscle
atrophy
- Hyperadrenocorticism &
Hypothyroidism => Muscle
atrophy
- Nutritional
- White Muscle Disease
- Economic importance in
young Cattle, Sheep & Pigs (also foals)
- Se &/or Vit. E deficiency
- Grossly:
- Lesions are bilaterally
symmetrical (hard working
muscles)
- Pigs: lesions in heart & liver
- Pigs: lesions in heart & liver
- Lesions are bilaterally
symmetrical (hard working
muscles)
- Pathogenesis:
- Oxygen free radicals (OFR)
can damage cell membranes
- Vit. E involved in binding
OFR & Glutathione
peroxidase (includes Se)
=> Neutralizes effects of
OFR
- If Vit. E & Se deficient: Balance shifts
to membrane damage => Ca2+ entry
& mitochondrial damage => cell
swells & dies
- Vit. E involved in binding
OFR & Glutathione
peroxidase (includes Se)
=> Neutralizes effects of
OFR
- Oxygen free radicals (OFR)
can damage cell membranes
- Economic importance in
young Cattle, Sheep & Pigs (also foals)
- White Muscle Disease
- Exertional
- Caused by intensive &
exhaustive activity of major
muscle masses
- Classically occurs in
the Horse after
unaccustomed exercise
- Equine exertional rhabdomyolysis
- Dissolution of striped
(skeletal) muscle
- Membrane damage &
leakage of myoglobin
- Myoglobinura = rhabdomyolysis
- Myoglobinura = rhabdomyolysis
- Membrane damage &
leakage of myoglobin
- Dissolution of striped
(skeletal) muscle
- Azoturia
- Exercise following
prolonged period of
rest
- Unable to move,
sweating, tremors
- Myoglobin leaks from muscle
cells -> leaks into urine -> urine is
dark red/brown (myoglobinuria) ->
damages renal tubules
- Exercise following
prolonged period of
rest
- Tying-up (similar to
Azoturia, but milder)
- Linked to
polysaccharide
storage myopathy
(many breeds)
- Ex. Equine polysaccharide
storage myopathy (EPSM)
- Ex. Equine polysaccharide
storage myopathy (EPSM)
- Capture myopathy,
Porcine stress
syndrome
- Caused by intensive &
exhaustive activity of major
muscle masses
- Toxic
- Neuromuscular Junction
- Myasthenia gravis (MG)
- 1) Acquired
- Autoimmune disease: Abs
directed against acetyl
choline receptors
- Associated w/ thymomas,
megaoesophagus &
hypothyroidism (Dogs)
- Autoimmune disease: Abs
directed against acetyl
choline receptors
- 2) Congenital
- Inherited deficiency in acetyl
choline receptors (Rare)
- No Abs against
acetyl choline
receptors in serum
- Inherited deficiency in acetyl
choline receptors (Rare)
- Both forms manifest as
weakness which worsens
on exercise
- 1) Acquired
- Botulism
- Due to ingestion of
Clostridium botulinum
toxin which inhibits
acetyl choline release
- Dx: Demonstrate toxin in
faeces, ingested material,
serum
- Due to ingestion of
Clostridium botulinum
toxin which inhibits
acetyl choline release
- Myasthenia gravis (MG)
- Neoplasia
- Rare in
domestic
animals
- Primary benign: Rhabdomyoma
- Primary malignant: Rhabdomyosarcoma
- Primary malignant: Rhabdomyosarcoma
- Metastases can also occur to
skeletal muscle (e.g. carcinoma,
haemangiosarcoma)
- Rare in
domestic
animals
- Inflammation: Myositis
- Anatomy
- Types of Myofibres
- Types of Myofibres
- Muscles of posture,
movement & respiration
- Bones function, structure & organization
- Bone is a hard, highly specialized connective
tissue, comprising interconnected cells
embedded in a clacified, collagenous matrix
- A living, dynamic, responsive
tissue, growing & remodeling
throughout life
- Functions:
- Supports movement
- Protects body
- Storage:
- Mineral bank
- Haematopoietic
stem cells
- Fat
- Fat
- Haematopoietic
stem cells
- Mineral bank
- Storage:
- Protects body
- Supports movement
- Structure:
- Composed of
cells & matrix
- Cells:
- Osteoblasts
- Mesenchymal cells of bone
marrow stromal origin
- Form the bone matrix (Osteoid)
- Form the bone matrix (Osteoid)
- Mesenchymal cells of bone
marrow stromal origin
- Osteoclasts
- Multinucleated cells
derived from
haematopoietic stem cells
- Responsible for bone resorption
- Responsible for bone resorption
- Multinucleated cells
derived from
haematopoietic stem cells
- Osteocytes
- Osteoblasts that have become
surrounded by mineralized
bone matrix
- Occupy cavities called lacunae
- Occupy cavities called lacunae
- Osteoblasts that have become
surrounded by mineralized
bone matrix
- Osteoblasts
- Matrix:
- Composed of type I
collagen & mineral
- Mineral - accounts for 65%
of bone (includes: Ca, P,
Mg, Mn, Zn, Cu & Na)
- Ground substance
(water, proteoglycans,
lipids)
- Strength
- Composed of type I
collagen & mineral
- Composed of
cells & matrix
- Bone Organization
- Not all bones are
organized in the
same way
- Organization dictated
by the pattern of
collagen deposition
- Organization dictated
by the pattern of
collagen deposition
- 1) Immature (Woven) Bone
- Collagen is arranged in a
"random weave"
- This is only
normal in the fetus
- In adults: Randomly woven
bone => sign of pathological
condition (e.g. fracture,
inflammation, neoplasia)
- In adults: Randomly woven
bone => sign of pathological
condition (e.g. fracture,
inflammation, neoplasia)
- This is only
normal in the fetus
- Collagen is arranged in a
"random weave"
- 2) Mature (Lamellar ) Bone
- The collagen is arranged in
orderly layers which are much
stronger than woven bone
- Two main types:
- Compact or cortical
bone
- forms the diaphyses of long
bones & the shell of all other
bones (contains Osteons)
- forms the diaphyses of long
bones & the shell of all other
bones (contains Osteons)
- Cancellous (spongy or
trabecular) bone
- occurs in vertebrae, flat
bones & epiphysyes of long
bones (Contains NO Osteons)
- occurs in vertebrae, flat
bones & epiphysyes of long
bones (Contains NO Osteons)
- Compact or cortical
bone
- The collagen is arranged in
orderly layers which are much
stronger than woven bone
- Not all bones are
organized in the
same way
- Periosteum
- A sheath of connective tissue
covering the bone (except at the
articular surfaces)
- The inner layer merges w/ the outer
layer of bone & contains
osteoblasts & stem cells
- The blood supply to the mature
bone enters via the periosteum
- Damage to the periosteum triggers
a hyperplastic rxn of the inner layer
- Damage to the periosteum triggers
a hyperplastic rxn of the inner layer
- The blood supply to the mature
bone enters via the periosteum
- The inner layer merges w/ the outer
layer of bone & contains
osteoblasts & stem cells
- A sheath of connective tissue
covering the bone (except at the
articular surfaces)
- Bone Development
- 2 Main Types:
- Intramembranous ossification
- Flat bones
mainly (e.g. skull)
- Mesenchymal cells
differentiate into osteoblasts
- There is NO cartilage
precursor template
- There is NO cartilage
precursor template
- Flat bones
mainly (e.g. skull)
- Endochondral ossification
- Long bones mainly
- Cartilage model of the
bone to be formed is
vascularised & replaced
by bone
- Long bones mainly
- Intramembranous ossification
- 2 Main Types:
- Physis (Growth plate)
- Esentially the remnant of the
cartilage model located at the
junction of Diaphysis & Epiphysis
- Imp. site: Many congenital or
nutritional bone diseases in the
growing animal manifest here
- In neonates & growing animals:
Growth plate is "open", i.e.
chrondrocyte proliferation balances
cell maturation & death
- The growth plate "closes" &
ossifies @ maturity
- The growth plate "closes" &
ossifies @ maturity
- Esentially the remnant of the
cartilage model located at the
junction of Diaphysis & Epiphysis
- Bone Resorption
- Mediated by PTH
& Calcitonin
- Parathyroid Hormone (PTH)
- Produced by chief cells in the
parathyroid glands
- Increases serum Ca2+
levels (released in response
to decreased serum Ca2+)
- Increases serum Ca2+
levels (released in response
to decreased serum Ca2+)
- STIMULATES
Osteoclasts
- Produced by chief cells in the
parathyroid glands
- Calcitonin
- Produced by C -cells
in the thyroid glands
- Decreases serum Ca2+
levels ( released in response
to Increased serum Ca2+)
- Decreases serum Ca2+
levels ( released in response
to Increased serum Ca2+)
- INHIBITS
Osteoclasts
- Produced by C -cells
in the thyroid glands
- Low serum Ca2+ -> Induces PTH secretion
-> Osteoclasts increase in # -> Attach to
bone & resorb mineralized matrix => Serum
Ca2+ INCREASES
- Mediated by PTH
& Calcitonin
- Bone Dynamics
- Bone growth & maintenance of normal
structure are directly related to
mechanical forces which generate
bioelectrical potentials (piezoelectricity)
- These potentials strengthen bone
while inactivity reduces them,
leading to bone loss
- These potentials strengthen bone
while inactivity reduces them,
leading to bone loss
- Neonates: Bone growth
predominates & modeling is Imp.
- Adults: Formation of bone is balanced
by resorption (remodeling)
- Adults: Formation of bone is balanced
by resorption (remodeling)
- Bone resorption may exceed
formation in pathological
stages (Hormonal, trauma,
nutritional) or in old age &
disuse
- Bone growth & maintenance of normal
structure are directly related to
mechanical forces which generate
bioelectrical potentials (piezoelectricity)
- Bone is a hard, highly specialized connective
tissue, comprising interconnected cells
embedded in a clacified, collagenous matrix
- Pathology of Bone
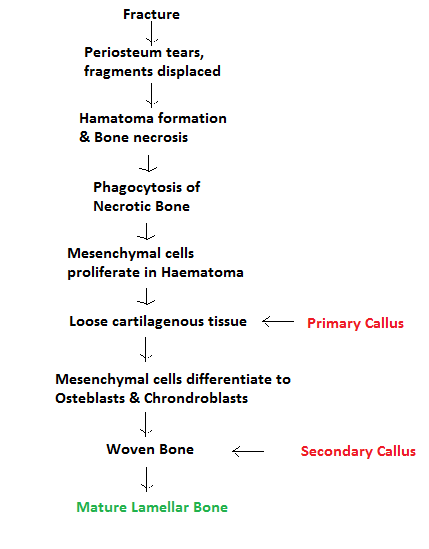
- Fractures
- Traumatic
- Normal bone broken by
excessive force
- Normal bone broken by
excessive force
- Pathological
- Abnormal bone broken by
minimal or no trauma
- Abnormal bone broken by
minimal or no trauma
- Fracture Repair
- Callus
- Bridges the gap,
Encircles fracture site,
Stabilizes fracture
- Bridges the gap,
Encircles fracture site,
Stabilizes fracture
- Factors which delay healing:
- Malnutrition
- Inadequate blood supply
(leads to hypoxia)
- Leads to excess
cartilage in Callus
- Healing can still
occur since this
can turn to bone
- Healing can still
occur since this
can turn to bone
- Excess movement
- Leads to excess
fibrous tissue in Callus
- This forms a false
joint & can't heal
properly
- This forms a false
joint & can't heal
properly
- Presence of Necrotic bone
(may form a sequestrum)
- Bacterial Infection
- Bacterial Infection
- Leads to excess
fibrous tissue in Callus
- Leads to excess
cartilage in Callus
- Inadequate blood supply
(leads to hypoxia)
- Malnutrition
- Traumatic
- Metabolic Bone Diseases
- Manifestation of Systemic Disease
in the skeleton (Endocrine,
Nutritional or Toxic Origin)
- Hyperparathyroidism (Fibrous
Oesteodystrophy)
- Bone is resorbed & replaced
by Fibrous, "rubbery"
connective tissue
- Caused by: Persistently elevated PTH
- Caused by: Persistently elevated PTH
- Causes of Increased PTH:
- Primary (Rare)
- Increased production of PTH NOT
related to Ca2+ or P levels (i.e.
autonomous)
- Due to parathyroid neoplasia or bilateral
idiopathic parathyroid hyperplasia
- Results in => Hypercalcaemia
- Results in => Hypercalcaemia
- Due to parathyroid neoplasia or bilateral
idiopathic parathyroid hyperplasia
- Increased production of PTH NOT
related to Ca2+ or P levels (i.e.
autonomous)
- Secondary (much
more common)
- Renal
- Chronic renal failure
(Reduced perfusion)
- => Retention of P ( & inadequate
production of Vit. D by kidneys)
- Hyperphosphataemia &
Hypocalcaemia (High P
depresses Ca2+)
- Low Ca2+ => PTH production
=> Increased Ca2+ resorption
from bone ("Rubber jaw")
- => Fibrous Osteodystrophy
- Low Ca2+ => PTH production
=> Increased Ca2+ resorption
from bone ("Rubber jaw")
- Hyperphosphataemia &
Hypocalcaemia (High P
depresses Ca2+)
- => Retention of P ( & inadequate
production of Vit. D by kidneys)
- Chronic renal failure
(Reduced perfusion)
- Nutritional (Poor diet) -
"Rubber Jaw"
- Low Ca2+/ High P diets/
Vit. D deficiency
- Increased Osteoclastic resorption
of bone & deposition of fibro-osteoid
matrix that fails to mineralize
- Flat bones of the skull (Maxillary
& Nasal bones) => Swell
- Long bones become soft w/
thin cortices (fracture easily)
- Long bones become soft w/
thin cortices (fracture easily)
- Flat bones of the skull (Maxillary
& Nasal bones) => Swell
- Increased Osteoclastic resorption
of bone & deposition of fibro-osteoid
matrix that fails to mineralize
- Ex: Horses - Grain/corn/bran
- Swine - Fed grain rations
- Dogs & Cats - Fed meat only diets
- Dogs & Cats - Fed meat only diets
- Swine - Fed grain rations
- More common in
young, fast growing
animals (w/
exception of horses)
- Low Ca2+/ High P diets/
Vit. D deficiency
- PTH secretion
triggered by Decreased
plasma Ca2+
- Renal
- Paraneoplastic
- Parathyroid hormone-
related protein produced by
certain neoplasms
- Parathyroid hormone-
related protein produced by
certain neoplasms
- Primary (Rare)
- Bone is resorbed & replaced
by Fibrous, "rubbery"
connective tissue
- Osteoporosis
- a LESION, not a
distinct disease entity
- Reduction in bone
quantity, not quality
- Bone resorption exceeds formation
-> Pathological loss of bone
- The bone that remains is
normally mineralized (Just not enough of it)
- => Prone to fractures due
to reduced strength
- => Prone to fractures due
to reduced strength
- The bone that remains is
normally mineralized (Just not enough of it)
- Bone resorption exceeds formation
-> Pathological loss of bone
- Causes:
- Starvation, nutritional
deficiency (Ca2+)
- Senility
- Physical inactivity (Disuse)
- Physical inactivity (Disuse)
- Farm animals (Most
common cause)
- Calves on indigestible
milk replacer
- Cattle on low quality hay
in cold climates
- Cattle on low quality hay
in cold climates
- Calves on indigestible
milk replacer
- Senility
- Starvation, nutritional
deficiency (Ca2+)
- Localized or general
- Bone atrophy
or osteopaenia
- a LESION, not a
distinct disease entity
- Rickets
- Disease of the young, fast
growing skeleton
- Pathogenesis:
- Failure of mineralization of
Physeal & Epiphyeal cartilage
during endochrondral ossification &
of newly formed osteoid
- Failure of mineralization of
Physeal & Epiphyeal cartilage
during endochrondral ossification &
of newly formed osteoid
- Due to diets low in Vit. D
(or P - less common)
- Vit. D. maintains normal
plasma levels of Ca2+ & P
(acts on intestines, bones,
kidneys)
- Calcitriol enhances
GI absorption of Ca
& P
- w/o Vit. D, only 10-15% of
dietary Ca2+ is absorbed
- w/o Vit. D, only 10-15% of
dietary Ca2+ is absorbed
- Calcitriol enhances
GI absorption of Ca
& P
- Vit. D. maintains normal
plasma levels of Ca2+ & P
(acts on intestines, bones,
kidneys)
- Growth plates are thickened
- As the zone of proliferation does not mineralize
& mature => blood vessels & chondroclasts
cannot invade so the cartilage is not removed
- As the zone of proliferation does not mineralize
& mature => blood vessels & chondroclasts
cannot invade so the cartilage is not removed
- Metaphyses are flared
- Because bone & cartilage cannot be removed
(Osteoclasts cannot bind to poorly mineralized
bone -> further accentuated by weight bearing)
- Because bone & cartilage cannot be removed
(Osteoclasts cannot bind to poorly mineralized
bone -> further accentuated by weight bearing)
- Enlarged costochondral
junctions
- Disease of the young, fast
growing skeleton
- Osteomalacia
- Similar to Rickets,
except disease of adult
skeleton
- Failure of newly formed
osteoid to mineralize
- Similar to Rickets,
except disease of adult
skeleton
- Others
- Hormone -related (Hormones
which directly affect bone growth
& resorption - other than PTH &
Calcitonin)
- Insulin, Growth hormone (Somatotrophin),
Glucocorticoids, Oestrogens, Androgens &
Thyroid Hormones
- Insulin, Growth hormone (Somatotrophin),
Glucocorticoids, Oestrogens, Androgens &
Thyroid Hormones
- Vitamin -Related Conditions
- Vitamin A
- Hypervitaminosis A
- Cats fed liver for
prolonged periods
- Vertebrae fuse (Vertebral ankylosis)
with each other due to bone
proliferation (esp. in neck)
- Pathogenesis not clear
- Pathogenesis not clear
- Can also be teratogenic
-> Cleft palate
- Cats fed liver for
prolonged periods
- Hypovitaminosis A
- Due to dietary deficiency in
Dam: Can be teratogenic in
Pigs & large Cats
- More commonly, due to dietary
deficiency in Neonates (Puppies,
Kittens, Calves, Piglets)
- Deficiency => Failure of osteoclastic
remodeling => Bone overgrowth &
nerve compression (esp. optic
nerves)
- Due to dietary deficiency in
Dam: Can be teratogenic in
Pigs & large Cats
- Essential for normal
bone growth in
foetuses & neonates
- Stimulates osteoclasts
- Stimulates osteoclasts
- Hypervitaminosis A
- Hypervitaminosis D
- Dietary or
iatrogenic origin
- Usually chronic
- Hypercalcaemia: Metastatic
calcification of soft tissues
- Dietary or
iatrogenic origin
- Vitamin C (Ascorbic Acid)
- Scurvy in Pigs, NHPs
- Imp. for collagen
formation
- Haemorrhage
- Fractures
- Fractures
- Haemorrhage
- Scurvy in Pigs, NHPs
- Vitamin A
- Hormone -related (Hormones
which directly affect bone growth
& resorption - other than PTH &
Calcitonin)
- Manifestation of Systemic Disease
in the skeleton (Endocrine,
Nutritional or Toxic Origin)
- Inflammation
- Causes
- Bacteria (Most common)
- Viral, Fungal, Protozoal
(Less common)
- Staphy, Strep, A.
pyogenes, Gram -ve
- Viral, Fungal, Protozoal
(Less common)
- Bacteria (Most common)
- Routes of Infection
- Direct Inoculation
- At time of fracture
- At time of fracture
- Direct Extension
- From other infected sites
(sinuses, middle ear, joints)
- Arthritis, synovitis, otitis media,
rhinitis, sinusitis, meningitis or
tooth root abscess
- Arthritis, synovitis, otitis media,
rhinitis, sinusitis, meningitis or
tooth root abscess
- From other infected sites
(sinuses, middle ear, joints)
- Haematogenous
- Mostly young
farm animals
- Mostly young
farm animals
- Direct Inoculation
- Gross lesions
- Suppurative exudate (in bacterial
infection), Necrosis, Bone
proliferation, Pathological fractures
- Dead bone portions may be
separated from blood supply =>
forming bone sequestra
- Suppurative exudate (in bacterial
infection), Necrosis, Bone
proliferation, Pathological fractures
- Consequences
- Extension to adjacent bone
- Haematogenous spread to
other bones & soft tissue
- Possible consequence of
sepsis in young animals
- Salmonella dublin, A.
pyogenes, Strep
- Animal often dies of
sepsis prior to bone
lesions appearing
- Salmonella dublin, A.
pyogenes, Strep
- Possible consequence of
sepsis in young animals
- Pathologic features
- Draining fistulas,
necrosis & loss of
bone, new bone
- Draining fistulas,
necrosis & loss of
bone, new bone
- Sinus tracts to exterior
- Extension to adjacent bone
- Metaphyseal Osteopathy
- Idiopathic/ unknown cause
(Infectious aetiology ?)
- Young, fast growing Dogs
(Large or giant breeds)
- Distal radius & ulna most severely
affected: bilaterally symmetrical
- Swelling in metaphyses of long
bones (Neutrophilic infiltrate)
- Fever, lameness,
suppurative inflammation &
necrosis of metaphyses
- Fever, lameness,
suppurative inflammation &
necrosis of metaphyses
- Most resolve spontaneously, but
can progress to periosteal bone
proliferation
- May wax & wane
- May wax & wane
- Idiopathic/ unknown cause
(Infectious aetiology ?)
- Causes
- Neoplastic Bone Diseases
- Bone tissue:
- Osteoma
- Uncommon
- Horses & Cattle
- Flat bones (skull &
scapula)
- Disfigurement: Obstruct
nasal passages
- Recur if not completely removed
- Uncommon
- Osteosarcoma (OSA)
- Any neoplasm of
mesenchymal origin in which
the cells produce Osteoid
- Dogs & Cats
(Otherwise uncommon)
- Dogs: OSA(80%) > Chrondrosarcoma (10%) >
Fibrosarcoma/haemangiosarcoma (7%) >
Lymphoid & myeloid tumors of marrow
- Giant breeds of Dog are at
massively increased risk
- Strong site
preference (Dogs):
- Appendicular skeleton
3-4x more frequently
involved than axial
- Proximal humerus,
distal radius,
proximal tibia &
distal femur
- "Away from the elbow -
towards the knee"
- "Away from the elbow -
towards the knee"
- Proximal humerus,
distal radius,
proximal tibia &
distal femur
- Appendicular skeleton
3-4x more frequently
involved than axial
- Survival time is slightly
better for axial than
appendicular OSA (Dogs)
- Prognosis is poor due to
early metastasis
- Pulmonary metastases
- Bone metastases
- Pulmonary metastases
- Any neoplasm of
mesenchymal origin in which
the cells produce Osteoid
- Osteoma
- Cartilage:
- Chondroma
- Benign neoplasm
of cartilage
- Rare
- Slow growing, Expansile
w/ smooth border
- Benign neoplasm
of cartilage
- Chrondrosarcoma
- Any malignant neoplasm in
which mesenchymal cells
produce chondroid matrix
- Dogs (most
common), Sheep
- Flat bones
- Flat bones
- Slower growth rate, longer
clinical course & later to
metastasize than OSA
- Metastatic rate: 20%
- Any malignant neoplasm in
which mesenchymal cells
produce chondroid matrix
- Chondroma
- Bone tissue:
- Hyperostotic Bone Diseases
- Hypertrophic Pulmonary
Osteopathy (HPO)
- Periosteal proliferation of bone on
diaphyses & metaphyses of distal limbs
- Progressive & bilateral
- Most cases: Have
intrathoracic neoplasm or
chronic inflammatory focus
- Has also been associated w/
intra-abdominal lesions - Ex.
Botryoid rhabdomyosarcoma
in the canine urinary bladder
& ovarian tumors in Horses
- Has also been associated w/
intra-abdominal lesions - Ex.
Botryoid rhabdomyosarcoma
in the canine urinary bladder
& ovarian tumors in Horses
- Most cases: Have
intrathoracic neoplasm or
chronic inflammatory focus
- Progressive & bilateral
- Periosteal proliferation of bone on
diaphyses & metaphyses of distal limbs
- Craniomandibular Osteopathy
- West Highland
terriers & Scottish
terriers
- Puppies: Arises @
4 -7 months
- Puppies: Arises @
4 -7 months
- Bilaterally symmetrical
periosteal proliferation of
new bone
- Irregular thickening of
rami of mandibles &
skull bones (tympanic bullae)
- West Highland
terriers & Scottish
terriers
- Hypertrophic Pulmonary
Osteopathy (HPO)
- Developmental Bone Diseases
- Primary abnormalities of Bone,
Cartilage or Mesenchyme
- Hereditary or Environmental
- Localized or Generalized
- Generalized
- Proportionate Dwarfism
- Minature breeds: Due to
growth factor deficit
- Minature breeds: Due to
growth factor deficit
- Chondrodysplasia
- Abnormal cartilage
formation
- Cattle, Dogs, Sheep,
Pigs & Cats
- Affects bones which form from a
cartilage model (endochondral
ossification) - long bones are shorter
than normal
- Leads to Disproportionate Dwarfism
- Leads to Disproportionate Dwarfism
- Affects bones which form from a
cartilage model (endochondral
ossification) - long bones are shorter
than normal
- Localized forms occur in some
Dogs as a breed associated
characteristic (e.g. affecting
skulls of Pekingnese & Bulldogs
or the limbs of Dachshunds &
Basset hounds)
- Abnormal cartilage
formation
- Osteopetrosis (Marble
bone disease)
- Hyperactive osteoblasts/ Failure of
resorption by osteoclasts => Failure
of remodeling of cancellous bone
- Bones become thickened
& dense, but brittle
- Associated w/ viral
infections (e.g. FeLV, BVD)
- Hyperactive osteoblasts/ Failure of
resorption by osteoclasts => Failure
of remodeling of cancellous bone
- Proportionate Dwarfism
- Localized
- Cervical Vertebral Stenotic
Myelopathy (Wobblers)
- Equine disease
- Narrowing of the vertebral canal
due to vertebral malalignment or
maldevelopment
- Fast growing males ranging
from 8 months to 4 yrs
- Hind limb ataxia: Due to cord
compression
- Hind limb ataxia: Due to cord
compression
- Fast growing males ranging
from 8 months to 4 yrs
- Dogs: Great
dane, Doberman
- Static: C5-C7
(1-4yrs)
- Dynamic: C3 -C5
(1 yr)
- Equine disease
- Angular Limb Deformity
- Lateral deviation of distal
portion of limb (usually)
- Most common in foals:
Congenital or Acquired
- Causes: Malpositioning (in utero),
excessive joint laxity, hypothyroidism,
trauma, overnutrition, defective
endochrondral ossification
- Causes: Malpositioning (in utero),
excessive joint laxity, hypothyroidism,
trauma, overnutrition, defective
endochrondral ossification
- Most common in foals:
Congenital or Acquired
- Lateral deviation of distal
portion of limb (usually)
- Cervical Vertebral Stenotic
Myelopathy (Wobblers)
- Generalized
- Primary abnormalities of Bone,
Cartilage or Mesenchyme
- Miscellaneous Bone Lesions
- Ossifying Pachymeningitis
- Plaques of bone form in the
Dura of the spinal cord
(especially in older dogs)
- No clinical
significance
- Plaques of bone form in the
Dura of the spinal cord
(especially in older dogs)
- Heterotopic Bone
- Spicules of bone
form in the lungs of
older dogs
- No clinical
significance
- Spicules of bone
form in the lungs of
older dogs
- Ossifying Epulides
- Neoplasms of
peridontal
fibroblast origin
- Occur in oral cavity
(esp. Boxers)
- Benign -> Complete
removal -> Good prognosis
- Neoplasms of
peridontal
fibroblast origin
- Ossifying Pachymeningitis
- Fractures
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.