420367
Beschreibung
Mindmap von melian.yates, aktualisiert more than 1 year ago
|
|
Erstellt von melian.yates
vor etwa 11 Jahre
|
|
Endocrine Pathology
- Pathogenic Mechanisms
of Endocrine Disease
- 1) Primary Gland Hypofunction
- Destruction of secretory cells by a
disease process (e.g. immune mediated
or other inflammatory injury in thyroids,
parathyroids or adrenal cortex)
- Failure of Gland development
(Hypoplasia or agenesis)
- Biochemical defect in synthetic
pathway of the hormone (usually genetic
aberrations & not commonly identifed in
vet species)
- Destruction of secretory cells by a
disease process (e.g. immune mediated
or other inflammatory injury in thyroids,
parathyroids or adrenal cortex)
- 2) Secondary Gland Hypofunction
- Destruction of glandular tissue or pituitary
leading to failure of secretion of trophic hormone
- => Hypofunction of target organ
- Ex. Endochronologically inactive pituitary
neoplasms interefere w/ secretion &
release of ACTH, TSH & FSH
- => Clinically detectable
hypofunction of adrenal
cortex, thyroid follicular
cells & gonads =>
Ensuing atrophy
- => Clinically detectable
hypofunction of adrenal
cortex, thyroid follicular
cells & gonads =>
Ensuing atrophy
- Ex. Endochronologically inactive pituitary
neoplasms interefere w/ secretion &
release of ACTH, TSH & FSH
- => Hypofunction of target organ
- Destruction of glandular tissue or pituitary
leading to failure of secretion of trophic hormone
- 3) Primary Gland Hyperfunction
- One of the Most Common
- Hyperplasia/neoplasia of
endocrine cells is involved
- The primary source synthesises &
secretes hormone autonomously at a
rate in excess of the ability of the body to
utilise & degrade th ehormone
- The primary source synthesises &
secretes hormone autonomously at a
rate in excess of the ability of the body to
utilise & degrade th ehormone
- One of the Most Common
- 4) Secondary Gland Hyperfunction
- Lesion in one gland causes excessive trophic
hormone secretion which results in long-term
hypersecretion in a target organ
- Ex. Canine ACTH-secreting pituitary tumor
=> Adrenal cortical hyperplasia/hypertrophy
& Hypercorticolism (Canine Cushing's
Syndrome)
- Ex. Canine ACTH-secreting pituitary tumor
=> Adrenal cortical hyperplasia/hypertrophy
& Hypercorticolism (Canine Cushing's
Syndrome)
- Lesion in one gland causes excessive trophic
hormone secretion which results in long-term
hypersecretion in a target organ
- 5) Hypersecretion of Hormones or
Hormone-like factors by non-endocrine tumors
- Ex. Adenocarcinoma of the anal
sac apocrine glands in Dogs
- Produces parathyroid hormone-related peptide
(PTHRP) => pseudo-hyperparathyroidism =>
Hypercalcaemia
- Produces parathyroid hormone-related peptide
(PTHRP) => pseudo-hyperparathyroidism =>
Hypercalcaemia
- Ex. Some canine lymphomas
(lymphosarcomas) may also exhibit a
similar effect (i.e. the tumor secretes or
is associated w/ a factor which induces
hypercalcaemia)
- Ex. Adenocarcinoma of the anal
sac apocrine glands in Dogs
- 6) Failure of Target cell response
- May be a failure of the
cell surface receptor
mechanism
- Lack of a 2nd
intracellular messenger
(e.g. cAMP) response
- Ex. Diabetes mellitus (Insulin resistance in
Obesity - receptor loss in connective tissue
cells, which then fail to react to insulin)
- May be a failure of the
cell surface receptor
mechanism
- 7) Endocrine Hyperactivity 2ndary to
disease in other organs
- Disease in one organ
results in hyperfunction of
an endocrine gland
- Ex. 2ndary hyperparathyroidism
associated w/ chronic renal failure
- Retention of phosphorous & alterations in
Vit. D metabolism lead to hypercalcaemia,
w/ resultant hyperparathyroidism & skeletal
demineralization
- Retention of phosphorous & alterations in
Vit. D metabolism lead to hypercalcaemia,
w/ resultant hyperparathyroidism & skeletal
demineralization
- Disease in one organ
results in hyperfunction of
an endocrine gland
- 8) Abnormal Hormone Degradation
- Decreased degradation: Can
manifest as Hypersecretion
- Increased degradation: May relate
to chronic drug administration
- Decreased degradation: Can
manifest as Hypersecretion
- 9) Iatrogenic Causes
- Long term administration of
hormones may lead to direct
or indirect effects
- Ex. Corticosteroid excess -> Cortisol ->
muscle weakness, calcinosis cutis, hair
loss & adrenal cortical atrophy
- Long term administration of
hormones may lead to direct
or indirect effects
- 1) Primary Gland Hypofunction
- Pituitary Gland
- Pituitary Cysts
- Pituitary Dwarfism (Juvenile
panhypopituitarism)
- Most common in German Shepards
- Most cases: Due to failure of the oropharnygeal
ectoderm to differentiate into pars distalis
- Associated w/ development of a pituitary cyst
- Signs become apparent at 2 months of age:
Retention of puppy coat progressing to bilaterally
symmetrical alopecia & hyperpigmented skin
- Signs become apparent at 2 months of age:
Retention of puppy coat progressing to bilaterally
symmetrical alopecia & hyperpigmented skin
- Associated w/ development of a pituitary cyst
- Most common in German Shepards
- Pituitary Dwarfism (Juvenile
panhypopituitarism)
- Neoplasia (Pituitary)
- ACTH secreting adenomas
- Most common in
the Dog
- Leads to syndrome of cortisol
excess (Cushing's syndrome)
- Most common in
the Dog
- Pars intermedia neoplasia (Horse)
- Although some tumors are endochrinologically
active, many of the features in equine disease are
associated w/ the compression effect on the
hypothalamus by the pituitary neoplasm
- Affects: seasonal shedding
of hair, appetite, body
temperature
- Although some tumors are endochrinologically
active, many of the features in equine disease are
associated w/ the compression effect on the
hypothalamus by the pituitary neoplasm
- Non-functional pituitary neoplasms
- Combination of atrophy of surrounding
pituitary & local extension into the brain can
cause a range of problemms
- => Weakness, collapse, blindness
- => Weakness, collapse, blindness
- Combination of atrophy of surrounding
pituitary & local extension into the brain can
cause a range of problemms
- Pituitary carcinoma
- Rare
- Usually endochronologically inactive
- Rare
- ACTH secreting adenomas
- Pituitary Cysts
- Adrenal Gland
- Hypofunction
- Hypoadrenocorticism (Addison's Disease)
- Can occur due to bilateral idiopathic
atrophy (immune mediated)
- Inflammation
- Bilateral Haemorrhage (sepsis related)
- Bilateral Haemorrhage (sepsis related)
- Inflammation
- Mineralocorticoid insufficiency
- Alterations in Na, K, Cl levels
- Can result in bradycardia
(Hyperkalaemia)
- Can result in bradycardia
(Hyperkalaemia)
- Alterations in Na, K, Cl levels
- Glucocorticoid insufficiency
- Hypoglycaemia
- Hypoglycaemia
- Can occur due to bilateral idiopathic
atrophy (immune mediated)
- Hypoadrenocorticism (Addison's Disease)
- Hyperfunction
- Canine Cushing's Disease
- Most common cause: functional
corticotroph pituitary gland adenoma =>
Bilateral adrenal gland hyperplasia
- Note: Severity of the
syndrome bears no relation to
the size of the neoplasia
- Less common cause (10-15% cases): Functional
adrenal gland neoplasia
- Pathogenesis: Gluconeogenesis ,
protein catabolism, lipolysis &
anti-inflammatory effects due to
glucocorticoids
- => Weakening of muscles (trembling,
lordosis, pendulous abdomen, atrophy of
temporal muscles)
- => Hepatomegaly (Due to steroid
hepatopathy - increased deposits of lipid &
glycogen)
- => Skin lesions (Atrophy of epidermis &
adnexae, cutaneous calcification -30%
cases - Ca is deposited along dermal
connective tissue fibres & can penetrate
the already atrophied skin)
- => Calcification in lungs, muscle & stomach
- => Increased appetite (Direct effect of
cortisol &/or destruction of appetite centre in
hypothalamus)
- => Increased appetite (Direct effect of
cortisol &/or destruction of appetite centre in
hypothalamus)
- => Calcification in lungs, muscle & stomach
- => Skin lesions (Atrophy of epidermis &
adnexae, cutaneous calcification -30%
cases - Ca is deposited along dermal
connective tissue fibres & can penetrate
the already atrophied skin)
- => Hepatomegaly (Due to steroid
hepatopathy - increased deposits of lipid &
glycogen)
- => Weakening of muscles (trembling,
lordosis, pendulous abdomen, atrophy of
temporal muscles)
- Most common cause: functional
corticotroph pituitary gland adenoma =>
Bilateral adrenal gland hyperplasia
- Canine Cushing's Disease
- Adrenal Hyperplasia
- Nodular hyperplasia of Cortex (Common)
- Usually multiple &
bilateral (Dog, Cat,
Horse)
- Usually multiple &
bilateral (Dog, Cat,
Horse)
- Diffuse Hyperplasia
- Seen w/ functional
tumors of pituitary
gland
- Seen w/ functional
tumors of pituitary
gland
- Nodular hyperplasia of Cortex (Common)
- Adrenal Neoplasia
- Cortical adenomas
- Often incidental finding
- May arise in glands w/
existing nodular hyperplasia
- Often incidental finding
- Cortical Carcinomas
- Less common than
adenoma
- Can be bilateral
- If functional, these tumors will
result in marked atrophy of the
contralateral gland
- Clinical signs: as described for
Cushing's disease + the potential
for invasion of major vessels &
distant metastases
- Clinical signs: as described for
Cushing's disease + the potential
for invasion of major vessels &
distant metastases
- If functional, these tumors will
result in marked atrophy of the
contralateral gland
- Cattle & Dogs >
Other species
- Less common than
adenoma
- Medullary
phaeochromocytoma
- Cattle & Dogs > other
species
- Can be large & invade locally to
caudal vena cava plus distant
metastases
- Some may be functional w/ signs
relating to adrenaline/noradrenaline
excess => Tachycardia, Cardiac
hypertrophy
- Some may be functional w/ signs
relating to adrenaline/noradrenaline
excess => Tachycardia, Cardiac
hypertrophy
- Cattle & Dogs > other
species
- Cortical adenomas
- Hypofunction
- Endocrine Pancreas
- Diabetes Mellitus
- Aetiology
- Relative or absolute lack of Insulin from
pancreatic Beta cells (i.e. hypofunction)
- Destruction of islet cells
secondary to pancreatitis
- The exocrine pancreas initially is
inflamed, the rxn spreads to &
involves the islets of Langerhans
- Condition can be chronic &
relapsing, with gradual replacement
of pancreatic tissue by fibrosis
- Condition can be chronic &
relapsing, with gradual replacement
of pancreatic tissue by fibrosis
- The exocrine pancreas initially is
inflamed, the rxn spreads to &
involves the islets of Langerhans
- Amyloid Deposition in Islets of
Langerhan(Cats)
- Note: Older Cats often have
scattered amyloid deposits in islets
w/o signs of diabetes mellitus
- Note: Older Cats often have
scattered amyloid deposits in islets
w/o signs of diabetes mellitus
- Idiopathic Pancreatic Atrophy
- Hypoplasia
- Destruction of islet cells
secondary to pancreatitis
- Relative or absolute lack of Insulin from
pancreatic Beta cells (i.e. hypofunction)
- Pathology
- Reduced availability of Insulin -> Hyperglycaemia
- Weight loss & weakness
- Reduced resistance to infection
(Leukocyte function is impaired)
- Hepatic fatty change (can lead
to cirrhosis in some cases)
- Cataracts -> bilateral lens opacity (due
to sorbitol pathway metabolism of
glucose by the lens)
- Renal glomerular sclerosis (Deposits of
glycoprotein in the glomeruli)
- Renal glomerular sclerosis (Deposits of
glycoprotein in the glomeruli)
- Cataracts -> bilateral lens opacity (due
to sorbitol pathway metabolism of
glucose by the lens)
- Hepatic fatty change (can lead
to cirrhosis in some cases)
- Reduced resistance to infection
(Leukocyte function is impaired)
- Weight loss & weakness
- Reduced availability of Insulin -> Hyperglycaemia
- Common in Dogs
(esp. Females)
- Aetiology
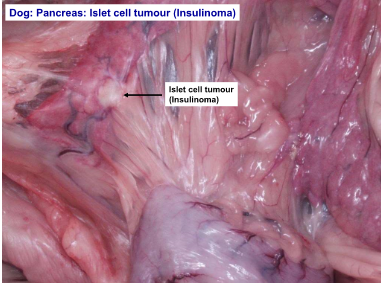
- Endocrine Pancreatic Neoplasia
- Insulinoma
- Neoplasia of pancreatic
Beta cells
- Carcinomas are more common than adenomas
- Usually functionally active -> Marked systemic effects
- Functional tumors
=> Hypoglycaemia
- Over time, hypoglycaemia =>
Neuronal necrosis
- Over time, hypoglycaemia =>
Neuronal necrosis
- More common in duodenal limb of pancreas
- Weakness, ataxia, altered temperament
(which can progress to seizures & collapse)
- Weakness, ataxia, altered temperament
(which can progress to seizures & collapse)
- Functional tumors
=> Hypoglycaemia
- Usually functionally active -> Marked systemic effects
- Neoplasia of pancreatic
Beta cells
- Gastrinoma
- Uncommon
compared to
insulinoma
- Gastrin causes hypersecretion of gastric acid ->
Ulceration of gastrointestinal mucosa
- Vomiting, diarrhoea & weight loss
- Invade pancreas, then spread to lymph nodes & liver
- Invade pancreas, then spread to lymph nodes & liver
- Vomiting, diarrhoea & weight loss
- Uncommon
compared to
insulinoma
- Glucagonoma
- Rare
- Glucagon induces hyperglycaemia
- Rare
- Insulinoma
- Diabetes Mellitus
- Thyroid Gland
- Develomental Disorders
- Accessory thyroid tissue
- Common
- Remnants of embryological
development of thyroid gland
- Usually in mediastinum,
often in heart base area
- Usually in mediastinum,
often in heart base area
- Common
- Thyroglossal Duct Cysts
- In ventral cervical region, fluctuant cysts
- Can become neoplastic
- Can become neoplastic
- In ventral cervical region, fluctuant cysts
- Accessory thyroid tissue
- Hypothyroidism
- Imp. in Dog (Uncommon
in other species)
- Idiopathic follicular atrophy
- Slowly progressive
replacement of the gland by
adipose tissue
- Slowly progressive
replacement of the gland by
adipose tissue
- Lymphocytic thyroiditis
- Lymphocytic infiltration into the
gland as a consequence of
autoantibody formation
- Lymphocytic infiltration into the
gland as a consequence of
autoantibody formation
- Extrathyroidal Effects of
Hypothyroidism
- Reduced BMR
- Skin
- Bilaterally symmetrical alopecia
(esp. tail & neck area)
- Hyperkeratosis & Hyperpigmentation
- Myxoedema can lead to thickening of the skin
(due to dermal accumulation of
glycosaminoglycans & hyaluronic acid)
- Bilaterally symmetrical alopecia
(esp. tail & neck area)
- Reproductive system
- Reduced sperm count, reduced/absent oestrus
- Reduced sperm count, reduced/absent oestrus
- Metabolic alterations
- Marked increase in cholesterol levels, which in
turn can lead to enlarged liver, atherosclerosis &
glomerular & corneal lipidosis
- Marked increase in cholesterol levels, which in
turn can lead to enlarged liver, atherosclerosis &
glomerular & corneal lipidosis
- Reduced BMR
- Imp. in Dog (Uncommon
in other species)
- Hyperthyroidism
- Common in Cats
- Even w/ functional thyroid neoplasia in Dogs, it is
uncommon to see hyperthyroidism since they are
more able to excrete excess thyroid hormones
- Even w/ functional thyroid neoplasia in Dogs, it is
uncommon to see hyperthyroidism since they are
more able to excrete excess thyroid hormones
- Polyuria, Polydypsia, Polyphagia
- Weight loss
- Hyperexcitability
- Heat intolerance
- Cardiac alterations (Hypertrophic
cardiomyopathy, Tachycardia,
Dysrhythmia)
- Cardiac alterations (Hypertrophic
cardiomyopathy, Tachycardia,
Dysrhythmia)
- Heat intolerance
- Hyperexcitability
- Weight loss
- Common in Cats
- Thyroid Gland Hyperplasia
- Goitre
- Non-neoplastic, non-inflammatory
enlargement of the thyroid gland
- Diffuse goitre occurs in animals w/
an iodine deficient diet
- Non-neoplastic, non-inflammatory
enlargement of the thyroid gland
- Nodular Hyperplasia
- Multiple small nodules within the gland
- Usually functional in the Cat (rarely
functional in other species)
- Multiple small nodules within the gland
- Goitre
- Thyroid Gland Neoplasia
- Follicular adenoma
- Discrete capsule & usually solitary
(compare to nodular hyperplasia)
- More common in Cats
- Discrete capsule & usually solitary
(compare to nodular hyperplasia)
- Follicular Carcinoma
- Locally invasive & often metastasize
- Can arise in extrathyroidal tissue
- More common in Dogs
- Locally invasive & often metastasize
- C-cell Neoplasia
- Most common in Bulls
- Thought to relate to high Ca2+
diet causing stimulation of the
thyroid C-cells
- Thought to relate to high Ca2+
diet causing stimulation of the
thyroid C-cells
- May be found in association with
phaeochromocytomas & pituitary adenomas
(multiple endocrine neoplasia - MEN)
- Most common in Bulls
- Follicular adenoma
- Develomental Disorders
- Parathyroid Glands
- Hyperparathyroidism
- Primary Hyperparathyroidism
- Chief cell neoplasia
- Adenoma more common than carcinoma
- Most common in Dogs
- Often functional tumors (Increased levels of
PTH) => Bone resorption & hypercalcaemia
- May cause pathological fractures of the bones
- May cause pathological fractures of the bones
- Chief cell neoplasia
- Secondary Hyperparathyroidism
- Renal secondary hyperparathyroidism
- Nutritional secondary hyperparathyroidism
(Low Ca2+ &/or high P)
- Renal secondary hyperparathyroidism
- Pseudohyperparathyroidism
- Humoral hypercalcaemia of malignancy (e.g.
apocrine adenocarcinoma of anal sac,
lymphosarcoma, metastatic neoplasia to the bone)
- Humoral hypercalcaemia of malignancy (e.g.
apocrine adenocarcinoma of anal sac,
lymphosarcoma, metastatic neoplasia to the bone)
- Primary Hyperparathyroidism
- Hypoparathyroidism
- Most common in
small breed Dogs
- Usually caused by lymphocytic thyroiditis
- Clinical Signs (relate to consequences of
progressive decline in serum Ca2+):
Neuromuscular excitability
- Clinical Signs (relate to consequences of
progressive decline in serum Ca2+):
Neuromuscular excitability
- Note: Potential to
remove parathyroid
glands during surgery
- Most common in
small breed Dogs
- Hyperparathyroidism
- Chemoreceptor Organs
- Present at several sites (including carotid
& aortic bodies) in many areas of the body
-> Heart base tumors are most frequent
- Aortic body Adenoma & carcinoma
- Most common in Dogs
(brachycephalic breeds)
- Adenomas are more common than
carcinomas (most often seen as a mass of or
multiple nodules around the base of the heart)
- Carcinomas can invade the
pulmonary artery or atria (although
distant metastases are uncommon)
- They are non-functional, but can cause problems
due to their space occupying effect
- They are non-functional, but can cause problems
due to their space occupying effect
- Carcinomas can invade the
pulmonary artery or atria (although
distant metastases are uncommon)
- In addition to aortic body tumors, ectopic
thyroid tissue can cause tumor formation in the
region of the base of the heart
- Most common in Dogs
(brachycephalic breeds)
- Carotid body adenoma & carcinoma
- Arise near bifurcation of common carotid artery
- Due to proximity to the artery and nerves ->
excision/biopsy can be difficult
- Carotid body tumors tend to be more
malignant then aortic body
- Carotid body tumors tend to be more
malignant then aortic body
- Due to proximity to the artery and nerves ->
excision/biopsy can be difficult
- Arise near bifurcation of common carotid artery
- Multicentric tumors of chemoreceptor
tissue occur (esp. in brachycephalic
breeds)
- Present at several sites (including carotid
& aortic bodies) in many areas of the body
-> Heart base tumors are most frequent
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.