13671815
Beschreibung
Karteikarten von Jacky Chou, aktualisiert more than 1 year ago
|
|
Erstellt von Jacky Chou
vor mehr als 6 Jahre
|
|
| Frage | Antworten |
| What is meant by glaucoma? | Optic nerve neuropathy (nerve cell death), that is associated with increased IOP. It has a typical pattern of vision loss. |
| What are the main two types of glaucoma? (and their subtypes?) | 1. Open-angle glaucoma -Primary: presumed angle predisposition -Secondary: cells, inflammation 2. Closed-angle glaucoma (Acute angle -Primary: narrow anterior chamber angle -Secondary: tumours, synechiae |
| What happens in open-angle glaucoma? | Decreased aqueous drainage caused by dysfunction or microscopic clogging of the trabecular meshwork. This leads to chronically elevated IOP, and over many years, gradual vision loss. |
| What happens in close-angle glaucoma? | Narrowing or closure of the anterior chamber angle (irido-corneal juncture). Inadequate drainage of the aqueous humor leads to increased IOP and damage to the optic nerve. |
| What is the normal range of IOP? | 8~22mmHg (varies with corneal abnormalities) |
| What is the gold standard for asessing IOP? | Goldman Tonometry |
| What is the normal aqueous pathway | |
| What is gonioscopy and how does it work? | Using a goniolens (a special glass lens with mirrors on its side)allows us to look directly at the angle. When the glass lens is placed directly onto the cornea, the cornea-air interface reflection is broken (where it usually creates "total internal reflectin) and light from the angle can escape and be seen through the mirrors. |
| Eye Examination (4 key components when assessing for glaucoma) | 1. Intraocular Pressure 2. Angle Assessment 3. Optic Nerve 4. Visual Fields |
| Clinical features of closed-angle glaucoma: *History *Examination findings |
*History
Rapid onset pain
Blurring of vision
Light haloes
Nausea/vomiting
Headache
*O/E
Ciliary flush, hazy cornea (edematous), a mid-dilated pupil (reacting poorly to light).
Optic disc cupping (cup-to-disc ratio).
Image:
Image (binary/octet-stream)
|
| What is the immediate management (medical) of closed-angle glaucoma? [and how does each treatment work?] | Aim is to lower IOP. Urgent referral to ophthalmologist (ophthalmology emergency) 1. Reduce Aqeuous production: *Beta-blockerTopical -Timolol (Timoptol) *Alpha2-adrenergic agonist -Brimonidine (Alphagan) *Carbonic anhydrase inhibitor [CAI] -acetazolamide (Diamox) 2. Increase aqeuous OUTFLOW: Trabecular meshwork outflow *Miotics (pilocarpine), contricts pupil Uveoscleral outflow *Prostaglandin analogue (Latanoprost, bimatoprost) 3. Reduce vitreous volume: IV Mannitol, glycerol (osmotic agent) |
| Glaucoma Surgery What are the options? What do they do? | *Laser surgery YAG laser peripheral iridotomy: lasers a tiny hole in the peripheral iris to allow flow of aqueous humor. (Bypasses pupillary block) laser iridoplasty: lasers the periphery of the iris to contract it and pull it away from the angle. Laser trabeculoplasty: 60 laser spots are placed around 180 degrees of the trabecular meshwork, improves aq. drainage. *Surgery to improve aq. drainage Paediatrics Goniotomy: fine needle goniotomy knife introduced into ant. chamber, creates 120 degree incision around the trabecular meshwork. Trabeculotomy: external approach, with sclera flap and identify Schlemm's canal. Adult Lens surgery: cataract extraction Trabeculectomy: (most common procedure) Opening made through conjunctiva, sclera flap, enter ant. chamber, remove section of iris (partial iridectomy), close. Aq. collects around flap (bleb) and then drains into the tear film. Note: to prevent scarring use of anti-metabolites intraoperatively (5-Fluoroucil or Mitomycin-C) *Reduce Aqeous production Cytophotocoagulation/Cyclodiode laser *Drainage devices Molteno tube |
| What are the systemic side effects of a beta-blocker? | -bradycardia, HEART BLOCK, ASYSTOLE -HF -SOB and bronchospasm -APNEA in infants -CNS: confusion, delerium, depression -Impotence/decreased libido |
| Clinical features of open-angle glaucoma: *History *Examination | History: Symptoms are rare. (No pain, visiual disturbances). Usually detected on thorough ophthalm examination. |
| Risk factors for open-angle | *Age (increases with age) *Race (Blacks>whites) *Family history *HTN *Increased IOP *DM |
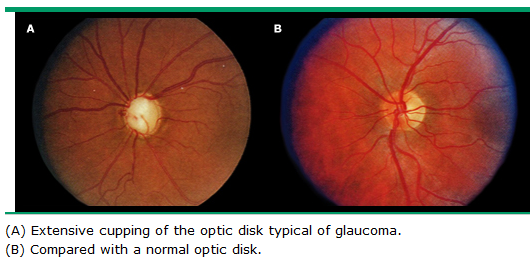
| What is optic nerve "cupping", and what is the cup-to-disc ratio? |
"Cupping" =Atrophy of the optic nerve head.
Image:
Image (binary/octet-stream)
|
| What is meant by retinal detachment? | Separation of the retina from the retinal pigment epithelium. |
| What is rhegmatogenous retinal detachment (RRD)? | Full thickness retinal hole or tear, allows fluid (from vitreous humour) to accumulate between the retina and RPE (subretinal space). |
| What are the clinical features of a rhegmatogenous retinal detachment? | Symptoms: flashes/floaters loss of vision (and/or shadow in the vision) Signs: Reduced vision (if macula) Peripheral field defect (on confrontation test) may have loss of red reflex. *Slit lamp: RBCs and pigment seen in vitreous, detachment can be seen with a fundal lens. |
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.