20000240
Beschreibung
Karteikarten von Marissa Alvarez, aktualisiert more than 1 year ago
|
|
Erstellt von Marissa Alvarez
vor etwa 5 Jahre
|
|
| Frage | Antworten |
| Endocrine: Growth Objectives | •Define the periods of growth and their characteristics •Understand the actions and the mechanisms of action for GH on bone and soft tissues •Role of IGF-1 (and IGF-II) •Describe the factors that control GH secretion •Examine the role of sex steroids •Define and understand the clinical symptoms associated with abnormalities in GH secretion |
| Endocrine Control of Growth GROWTH –Under influence of growth hormone: •Net synthesis of ___ •↑___ of the long bones •↑ size and number of ___ in soft tissues -Factors other than GH affect growth: •Genetics ->Inheritance ->Abnormalities can cause various developmental defects •Diet ->Malnourishment -> ↓ growth potential (__% brain development in first 2 years) ->Excess = ____, not growth •Freedom from disease and stressful environment ->Prolonged stress-induced secretion of ___ -> stunted growth (through protein break-down, ↓ __ ___ growth, inhibiting __ secretion) –Normal levels of growth-influencing hormones: •Thyroid hormone •Insulin •Sex hormones | proteins Length cells 70% OBESITY cortisol long bone GH |
| Growth Not continuous: –FETAL growth •___ hormones •Genetic/environmental factors determine ___ at birth •GH ___ involved –CHILDREN •Postnatal growth spurt: –1st _ years –After -> rate linearly ___ until puberty •Pubertal growth spurt (11 yrs for females, 13 yrs for males): –Marked ____ in linear growth –Cause not well-understood –Genetic/hormonal factors » _ androgens -> protein synthesis and bone growth »T from testes, adrenal androgens in ___ *BOTH _ & __ -> halt bone growth at end of puberty | Placental size NOT 2 declines acceleration ↑ females T (testosterone) & E2 (estradiol) |
| Metabolic Effects of GH NOT Related to Growth -GH is the MOST abundant ___ hormone secreted, even in adults, suggesting actions in ___ to growth -Exerts actions by binding ____ to target tissues -During prolonged FASTING or if energy requirements EXCEED available glucose stores: ->Adipose »Breakdown triglycerides -> ↑ [fatty acid]blood ->Skeletal muscles »↑ use of __ __ for fuel (glucose sparing) »_ glucose uptake [↑ [glucose]blood = conserved for glucose-dependent tissues (__ , __)] –>Liver » _ glucose output [↑ [glucose]blood = conserved for glucose-dependent tissues (__ , __)] ->Also stimulates ___ synthesis -> _ [amino acid]blood »May or may not be a direct action | anterior pituitary (AP) addition DIRECTLY ↑ fatty acids ↓ heart, brain ↑ protein ↓ |
| Growth Hormone Does NOT act ___ to exert effects on growth –Actions mediated by insulin-like growth factors (__ & __) •Structurally and functionally similar to insulin •Produced by many tissues •Have endocrine, paracrine, and autocrine actions •Act via __ ___ pathway | directly IGF-I & IGF-II tyrosine kinase |
| IGF-I –70 a.a. protein, synthesis stimulated by __ –Mediates GH’s growth-___ actions –Major source = ___ (released into blood) •Also produced locally by most other tissues (___) –> NOT released to blood –Is paracrine secretion a major factor during postnatal growth (first _ years) period? »Circulating [GH] and [IGF-I] are __ during this time –Control of PRODUCTION (other than by GH): •Nutrition: [↓ intake -> _ IGF-I (but _ GH)] •Age-related factors: ( _IGF-I accompanies _ GH at puberty -> pubertal growth spurt) •Tissue-specific stimulatory factors: –FSH/LH & sex steroids -> ↑ IGF-I within reproductive organs | GH promoting Liver paracrine 2 low ↓ ↑ ↑ ↑ |
| Growth Hormone IGF-II –Production NOT influenced by __ –Major source = ___ PRIMARY ROLE: •During FETAL development: –Receptors expressed very __ in development (in contrast, IGF-I receptors not expressed until later in fetal life) »Found in _____ cells (develops into the fetal portion of placenta) –Stimulates ___ growth –Stimulates both pre- and post-implantation embryonic growth In NEWBORNS: –IGF-II _, while IGF-I _ •Secreted during adulthood, but UNKNOWN role –Patients with tumors that secrete IGF-II develop ____ »Binds to insulin receptors @ ___ -67 a.a. -62% homology with IGF-1 -Immunologically ___ than IGF-1 | GH liver early trophoblast placental ↓ ↑ hypoglycemia (low blood sugar) liver different |
| Growth Hormone -GH (acting through __) stimulates growth in soft tissues and skeleton SOFT TISSUE –Hyperplasia (_ # cells) •↑ cell division •↓ apoptosis –Hypertrophy (↑ __ of cells) • _ protein synthesis –↑ amino acid uptake by cell –↑ activity of synthesis machinery »↑ DNA & RNA synthesis »↑ incorporation of amino acids into protein @ ribosome •↓ protein ____ | IGF-I ↑ size ↑ degradation |
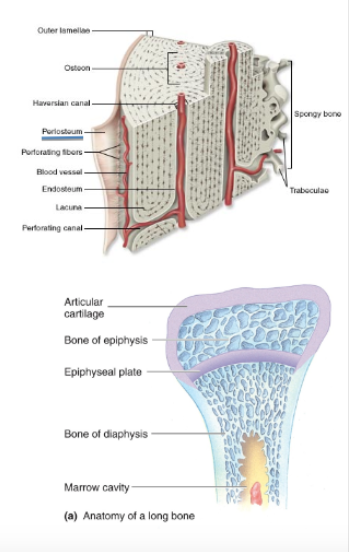
| Growth Hormone Effects on Skeletal Growth Effects on bone growth BONE STRUCTURE: ~____~ –Extracellular matrix composed of collagen fibers and semisolid gel »Responsible for tensile ___ of bone –CaPO4 precipitation -> bone ____ »Responsible for resistance to ____ ~____~ –Form bone by secreting osteoid ~_____~ –Dissolve bone tissues »Release minerals to blood •Relevant ANATOMY: –Periosteum »____ tissue surrounding bone –Diaphysis »___ of a long bone »Hollow, central cavity •Contains __ ___ –Epiphysis »“___” at either end of long bone •Where articulations are formed –___ ___ »Cartilaginous growth region b/w diaphysis and epiphysis | Osteoid strength hardening compression Osteoblasts ("Blasts Build Bone") Osteoclasts ("Clasts Cut bone") Connective Shaft bone marrow "knob" Epiphyseal plate |
| Bone Growth Ossification (bone ___) •Thickness: –Addition of new bone to surface of existing bone by osteo___ in the periosteum –Osteo___ along inner surface remove bone to enlarge marrow cavity | formation blasts ("osteoBlasts BUILD") clasts ("osteoClasts CUT") |
| Bone Growth LENGTH –Cartilage at ___ of epiphyseal plate is replaced with __: »Chondrocytes along epiphysis edge of epiphyseal plate multiply (temporary widening of ____ ___) »Older chondrocytes toward diaphysis _____ »Oldest hypertrophied cartilage is ____ »Chondrocytes die due to lack of access to ___ »Osteoclasts ___ away dead cells and calcified matrix »Osteoblasts move in (with blood supply) and ___ bone (____) | bottom bone epiphyseal plate hypertrophy calcified nutrients clear build (ossification) |
| Bone Growth LENGTH –Cartilage at ___ of epiphyseal plate is replaced with __: »Chondrocytes along epiphysis edge of epiphyseal plate multiply (temporary widening of ____ ___) »Older chondrocytes toward diaphysis _____ »Oldest hypertrophied cartilage is ____ »Chondrocytes die due to lack of access to ___ »Osteoclasts ___ away dead cells and calcified matrix »Osteoblasts move in (with blood supply) and ___ bone (____) | lacunae canaliculi Osteocytes matrix calcium parathyroid |
| Bone Growth Role of GH (via IGF-I) •Causes growth in both ___ and ___ • __ proliferation of epiphyseal cartilage • __ osteoblast activity –↑ length of long bones IF epiphyseal plate remains ____ »Sex hormones -> complete ____ (closure) •Normally at ___ | length thickness ↑ ↑ cartilaginous ossification puberty |
| REVIEW: Growth: -Factors affecting growth -Not continuous Growth Hormone: -Direct role in metabolism -Indirect role n growth -IGF-1 vs. IGF-2 GH on soft tissues: -via IGF-1 -hyperplasia & hypertrophy GH & Bone Growth: -cartilage cells (chondrocytes) -osteoclasts -osteoblasts -epiphyseal plate -Laying down of bone @ the epiphyseal plate | |
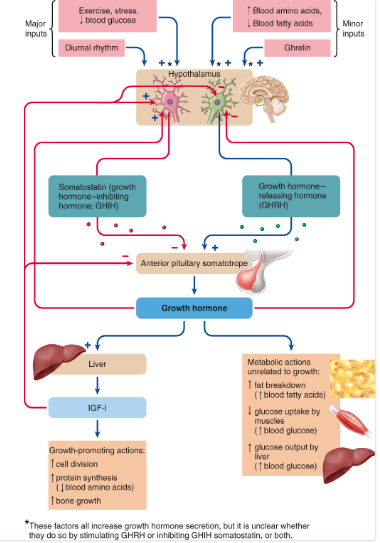
| Regulation of Secretion –GHRH and GHIH (____) •G-protein coupled receptors, with GHRH ____ and GHIH ____ cAMP •Negative feedback loops involve ____ of stimulatory factors and ____ of inhibitory factors –Factors affecting GH secretion •Displays ____ rhythm Recall that GH promotes ___ conservation for the brain: •Exercise & stress = __ [glucose]blood | somatostatin increasing decreasing inhibition stimulation diurnal glucose ↓ |
| GROWTH HORMONE During these extraneous situations: –↓ fat stores & ↑ body proteins • -> change in body composition –Away from ___ deposition –Toward muscle ____ (GH mary meditate effects of exercise) –If ↑protein meal -> _ [amino acid]blood -> _ GH secretion ->protein synthesis –↓ [fatty acid]blood -> _ GH secretion -> mobilizes fat -> ___ [fatty acid]blood –Ghrelin (from ___) -> _ GH secretion •Coordination of growth with nutrient acquisition | adipose hypertrophy ↑ ↑ ↑ stabilize stomach ↑ |
| GROWTH HORMONE Summary of regulation –Aimed at adjusting glucose, amino acids, and fatty acids –NO known ___-related signals influence growth hormone secretion •Levels of GH in early childhood, a period of accelerated growth, are ___ to those seen in adulthood •Why don’t soft tissues continue to grow under influence of GH? –GH may only be high enough during deep ___ »Time spent in deep sleep greatest during infancy and ___ with age »Time still spent in deep sleep in adulthood, yet we still ___ grow larger | growth similar sleep declines don’t |
| Growth Hormone DEFICIENCY Causes –Primary: ___ defect (lack __) –Secondary: ___ dysfunction (lack ___) Deficiency in CHILDHOOD: –Dwarfism » ___secretion of GH »Impeded skeletal growth -> short stature »Poorly developed muscles •_ protein synthesis »Excess subcutaneous fat stores •_ fat mobilization –Laron dwarfism »Abnormal ___ receptors •No response to __ •[GH]blood very ___ –GH adequate, but ___ is low (Target cell responsiveness to GH normal, but IGF-1 lacking) »Ex: African pygmies ___secretion during ADULTHOOD: –↓ skeletal muscle mass »↓ strength –↓ bone density »__ osteoblast activity during remodeling –↑ risk for ___ failure | Pituitary GH Hypothalamic GHRH Hypo ↓ ↓ GH GH high IGF Hypo ↓ heart |
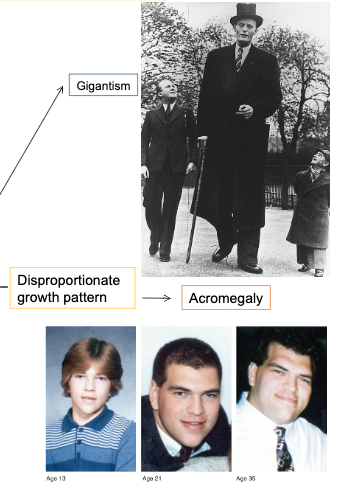
| Growth Hormone EXCESS Primary cause: –____ tumor of somatotropes •Symptoms dependent on ___ of onset: ->Childhood: (prior to epiphyseal plate ___) »Rapid growth in height without distortion of body proportions (____) –Post-adolescence: »No more ___ in height »Bones thicken •Extremities & face •Jaws and cheekbones become more ___ »Soft tissue proliferation •Skin, connective tissues »Hands and feet ___ •Fingers and toes thicken ->Disproportionate growth pattern (______) | Pituitary (somatotropes produce GH) age closure Gigantism growth prominent enlarge Acromegaly |
| Other Hormones Essential for Growth Thyroid Hormone: _____ •Not directly responsible for promoting growth •Stunted growth in ___thyroid children (but not opposite effect if hyperthyroid) •Insulin–Deficiency = ___ growth –Excess = excessive growth –Promotes protein synthesis –Structurally resembles __ (so interaction with IGF-I receptor is possible) •Androgens –Effects depend on presence of __ •Stimulate protein synthesis –Linear growth, weight gain, muscle mass ->Eventually, stop growth by promoting epiphyseal plate closure following conversion to ___ •Estrogens –Promote epiphyseal plate ___ •Other “poorly” understood peptide growth factors: –Stimulate mitotic activity in specific tissues (Ex: epidermal growth factor) | Permissive hypo blocks IGFs GH estrogen closure |
| SEX Differences in Growth •Puberty occurs ~ 2 years ___ in girls –Boys have ~ 2 more years of ___ •Average boy is ___ at beginning of the pubertal growth spurt than average girl •Greater ___-induced growth spurt in boys (↑ growth prior to plate closure) •Pubertal estrogen ↑ -> ↓ pubertal growth spurt (____ growth prior to closure) •_____ program brain for masculine GH secretion pattern (↑ cyclic peaks -> ↑ height in males) | earlier growth taller androgen Slowing Androgens |
| REVIEW Regulation of GH secretion: GHRH GHIH (somatostatin) Reytemincinty Exercise Stress Glucose Amino acids Fatty acids Ghrelin GH Disorders: Hyposecretion: Dwarfism (childhood) Laron Dwarfism (receptor insufficiency) Lack of IGF-1 (African Pygmies) Adulthood (minor symptoms) Hypersecretion: Gigantism Acromegaly Other hormones that influence growth: Thyroid, insulin, androgens, estrogens, peptide growth factors |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.