8845632
Description
Mind Map by Florence Papworth, updated more than 1 year ago
|
|
Created by Florence Papworth
over 7 years ago
|
|
Urine concentration
- Learning objectives
- Loop of Henle
- Countercurrent multiplier and distal tube
- Variable reabsorption of water
- mechanisms allowing urine to be concentrated to
an osmolarity higher than that of plasma
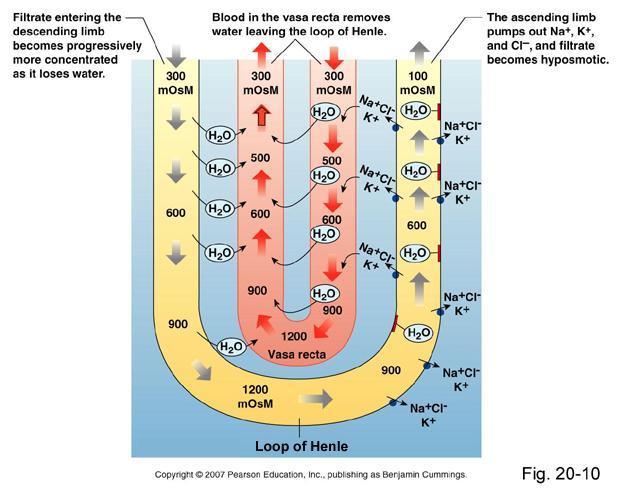
- Loop of Henle
- Countercurrent
multiplier
Annotations:
- a countercurrent system is a system which expends energy to create a concentration gradient. e.g. production of hyperosmotic urine by the kidney.
- loH essential for
formation of
concentrated urine
- maximum urine
concentration is related
to length of loH
- longer loH = higher
concentrated urine
- loH function - recover water
and sodium chloride from
urine
- loH function - recover water
and sodium chloride from
urine
- Loop of Henle
- Thick ascending limb
- impermeable to water and
urea. NaCl actively
reabsorbed
- impermeable to water and
urea. NaCl actively
reabsorbed
- Thin descending limb
- Permeable
to water
- Permeable
to water
- Thin ascending limb
- Impermeable to water.
Permeable to Na+ and
urea
- Impermeable to water.
Permeable to Na+ and
urea
- urine in descending limb
starts = 290 mosmol, in
ascending limbs finishes
90 mosmol
- Counter current flow - urine flow
opposite to blood flow of capillaries
supplied to tube
- In ascending limb -
movement of NA+, Cl-
and K+ out of tubular
lumen/into capillaries
using ATPase's.
Osmolarity decreases ~
100 mosmol/L
- In descending limb -
movement of water into
capillaries/ out of
tubular lumen
concentrates urine =
increases osmolarity >
1000mosmol/L
- Filtrate
HYPERTONIC at
turning point
- Fluid
HYPOTONIC in
ascending limb
- Fluid ISOTONIC as
enters descending
limb
- Isotonic, hypertonic etc filtrate =
compared to capillaries supplying
it
- osmolarity estabilished in renal medulla
- osmolarity estabilished in renal medulla
- Thick ascending limb
- Vasa recta
- countercurrent blood supply -
opposing flow direction to
filtrate
- prevents 'wash out' of
solutes
- 'picks up' water removed in
the loH
- also, picks up Na, Cl and K leaving
ascending limb
- also, picks up Na, Cl and K leaving
ascending limb
- countercurrent blood supply -
opposing flow direction to
filtrate
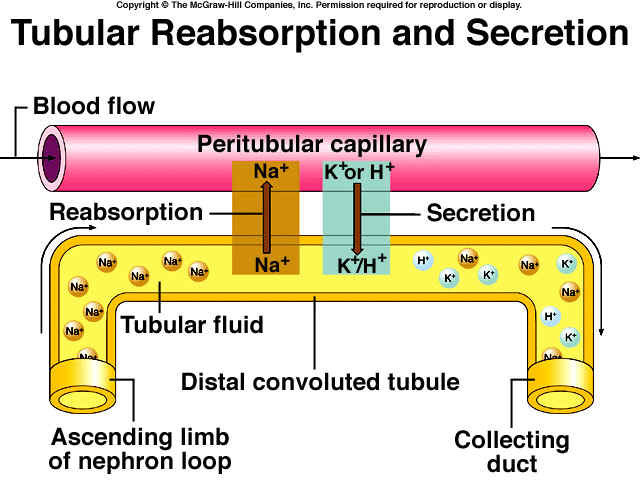
- Distal tubule
- Low and constant
permeability to water
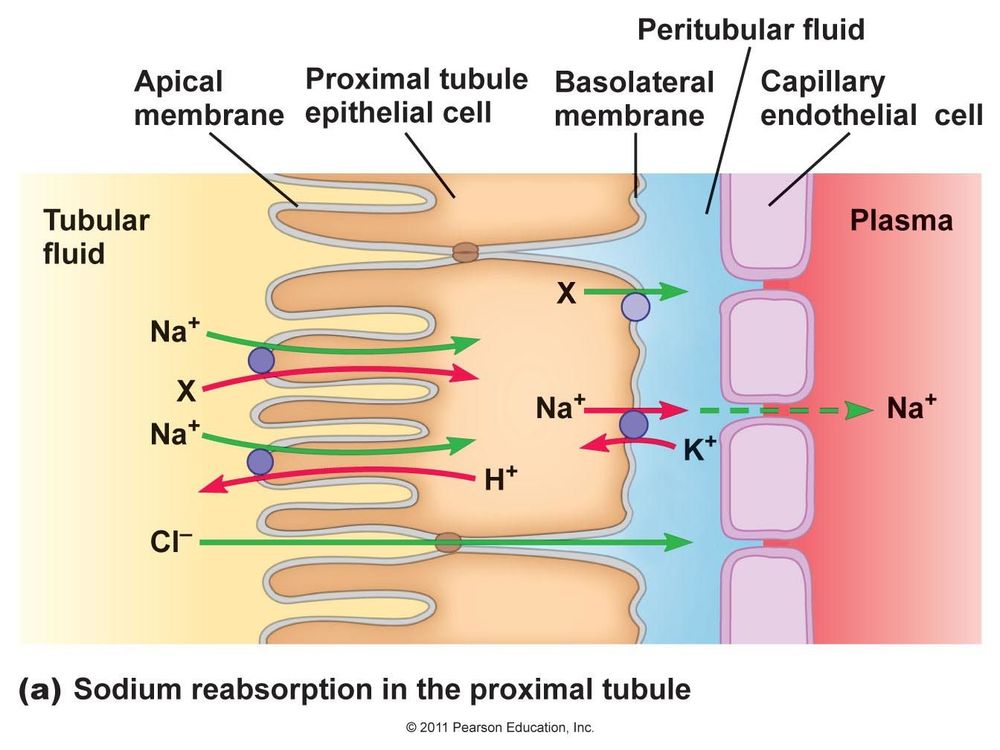
- Na+ and Cl-
reabsorption into
capillaries.
- via NaCl symporter in apical
membrane driven by
Na+K+ATPase in basal
membrane
- K+ and H+ moved
into the distal
tubule
- via NaCl symporter in apical
membrane driven by
Na+K+ATPase in basal
membrane
- Modification of distal tubule
where it passes close to
glomerulus -
JUXTAGLOMERULA APPARATUS
- regulates blood pressure and filtration rate of glomerulus
- regulates blood pressure and filtration rate of glomerulus
- Low and constant
permeability to water
- Collecting Duct
- By now, filtrate is
called urine
- runs parallel to ascending limb
of loH with flow in opposite
direction
- Both cortical and medullary
sections are IMPERMEABLE to
WATER, UREA and NACL
- Permeability of water
increases in prescense of
ANTIDIURETIC HORMONE
(ADH - vasopressin)
- approx 20% of glomerular
filtrate reaches collecting
duct
- 3/4 of water reaching collecting
duct is abstracted in cortical
collecting duct
- only 5% approx of glomerular
filtrate is reabsorbed in the
medulla
- 3/4 of water reaching collecting
duct is abstracted in cortical
collecting duct
- approx 20% of glomerular
filtrate reaches collecting
duct
- Collecting Duct - Principal cells
- Reabsorb Na+ into capillaries -
apicial ion channels -> capillaries
- Reabsorb Cl- into capillaries - driven by
luminal negative charge (Na+ actively moving
out)
- Secrete K+ - taken into lumen - ion
channels in apical membrane
- Variable permeability to water -
ADH dependant
- Variable permeability to water -
ADH dependant
- Secrete K+ - taken into lumen - ion
channels in apical membrane
- Reabsorb Cl- into capillaries - driven by
luminal negative charge (Na+ actively moving
out)
- Reabsorb Na+ into capillaries -
apicial ion channels -> capillaries
- By now, filtrate is
called urine
- Urea
- 1. Freely filtered in
descending limb, loH
- 2. 50% reabsorbed
in proximal tubule
- 3. Urea concentration
increases in loH
- 4. Tubular urea concentration
increases with removal of water NOT
urea
- 5. Reabsorption in
collecting duct in
presence of ADH
- 1. Freely filtered in
descending limb, loH
- Intercalated cells
- either bicarbonate or
H+ secreting
- Important in pH
regulation!
- Intercalated cells can
also reabsorb K+
- Secretes HCO3- or H+ from
capillary - tubule cell - lumen
- either bicarbonate or
H+ secreting
- KEY POINTS
- 1. Countercurrentmultiplier in loH - HYPEROSMOTIC medulla
- 2. Variable permeability of collecting
duct to water
- osmotic
reabsorption of
water
- variable urine
concentration
- osmotic
reabsorption of
water
- 3. Contribution of urea to
hyper-osmolarity in medulla
- 4. Cell types in collecting duct : principal cells
and intercalated cells
- 1. Countercurrentmultiplier in loH - HYPEROSMOTIC medulla
Media attachments
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.