22068810
Description
Flashcards by Evian Chai, updated more than 1 year ago
|
|
Created by Evian Chai
over 5 years ago
|
|
| Question | Answer |
| What are the 5 steps of respiration once air enters the body? | 1. Ventilation: exchange of air between atmosphere/alveoli 2. Exchange of O2/CO2 between alveolar air/blood in lung capillaries via diffusion 3. Bulk flow transports O2/CO2 through pulmonary/systemic circulation 4. Diffusion between blood in tissue capillaries/cells in tissue to exchange O2/CO2 5. Cellular utilisation of O2/CO2 production |
| What does the upper respiratory tract consist of? | The nasal cavity, the pharynx, the nostril, the mouth and the larynx |
| Where does the conducting zone end? | The terminal bronchioles |
| Where does the respiratory zone begin? | The respiratory bronchioles |
| What is the equation for rate of diffusion? | (area/thickness) * permeability |
| What are the 4 main functions of the lungs? | 1. Exchange of O2/CO2 2. Speech sounds 3. Immune defense 4. Regulate pH |
| What is: Tidal Volume Inspiratory Reserve Volume Expiratory Reserve Volume Residual Volume | Vt (500mL): normal volume of air inspired and expired IRV: (3000mL): Max amount of air lungs can inspire ABOVE Vt ERV (1200mL): Max amount of air lungs can expire ABOVE Vt RV (1200mL): Amount of air you cannot breathe out |
| What volume cannot be measured by the spirometer? | Residual volume |
| What is: Inspiratory Capacity Vital Capacity Functional Residual Capacity Total Lung Capacity | IC: Vt+ IRV (total amount you can breathe in) VC: IRV+Vt+ERV (total volume of air lungs can hold) FRC: ERV+EV (Volume in lungs AFTER NORMAL breath out) TLC: IRV+Vt+ERV+RV (total volume of lungs) |
| What is the difference between minute ventilation and alveolar ventilation? | Alveolar ventilation is the volume of FRESH air reaching alveoli/min, and takes into account dead space |
| What is the minute ventilation equation? | Ventilation Rate * Tidal Volume |
| What is the alveolar ventilation equation? | Minute ventilation - (ventilation rate * dead space volume) |
| What is the normal anatomical dead space? | 150mL |
| What is physiological dead space? | Anatomical+alveolar dead space |
| When Palv<Patm, [...] occurs When Palv>Patm, ... occurs When Palv=Patm, ... | 1. Inspiration 2. Expiraton 3. No net movement of air |
| Flow= | Flow= (Palv-Patm)/resistance |
| Intrapleural pressure is always.... and ... as chest wall expands | Negative becomes more negative |
| What is transpulmonary pressure equal to? | Palv-Pip |
| Resistance is mainly caused by... Upper airway resistance is caused by? | the airways Congestion in nose, pharynx, larynx |
| Why is resistance in the lower airways mainly caused by middle order bronchi? | Bronchiole resistences are in parallel |
| In quiet breathing, flow is [...] In high ventilation flow is ... | Laminar Turbulent |
| In asthma, resistance is caused by SM hypersensitivity to constrictors, leading to... | Bronchoconstriction |
| In chronic bronchitis, resistance is caused by...and... | Excess mucus production Inflammation |
| How does a change in radius impact resistance in series? | Resistance=1/r^4 so proportional increase to that |
| How does a change in radius affect resistance in parallel? | Total is (1/r1+1/r2+1/r3...) so increased individual resistance decreases total resistance |
| How does Adrenaline impact airway resistance? What about Ach? | Adrenaline is a dilator ACh is a constrictor |
| What is a physical factor on airway resistance during: 1. Inspiration 2. Expiration | 1. As PIp drops during inspiraton, LATERAL TRACTION from connective tissues increase the radius 2. Compression on airways during forced expiration decrease radius |
| Lung compliance is a measure of | how easily the lungs can stretch and expand aka how much work has to be done by muscles (higher=less work) |
| Lung compliance is measured by | Change in lung volume/change in transpulmonary pressure |
| What are the two factors determining lung compliance? | 1. Resistance of tissue to stretch 2. Surface tension |
| Does collagen or elastin impact the resistance of lung tissue to stretch? What does too much/too little of this result in? | The amount of elastin (not collagen because its not stretchable) Too much=low compliance=fibrosis Too little=high compliance=emphysema |
| How does surface tension influence lung compliance? | High surface tension lowers compliances because it opposes alveolar stretching |
| How does surfactant negate the impact of surface tension on lung compliance? | Surfactant lowers surface tension, increasing compliance |
| In smaller alveoli, a fall in radius results in greater resistance. How is this offsetted? | Surfactant secreted to lower ST and increase compliance |
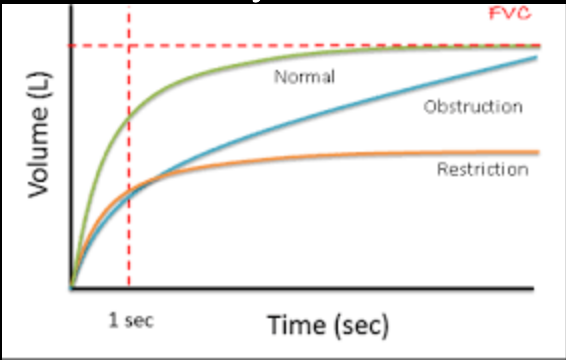
| The vitalgraph measures ... and ... The Forced Expiratory Ration (FER)=? | 1. Forced expiratory volume 2. Forced vital capacity 3. FEV1/FVC |
| Asthma, bronchitis and COPD are what type of lung disease and is indicated by what on the vitalograph? | Obstructive Lung Disease Unable to force out 75% in time period but can eventually reach max volume |
| cystic fibrosis, sarcoidosis, scoliosis, obesity, muscular dystrophy are what kind of lung disease, and are indicated by what on the vitalgraph? | 1. Restrictive Lung disease 2. Can force out 75% of max volume but unable to reach max volume |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.