1837084
Descrição
FlashCards por Anna Walker, atualizado more than 1 year ago
|
|
Criado por Anna Walker
quase 10 anos atrás
|
|
| Questão | Responda |
| How is colour vision assessed? | Using Ishihara colour plates. Ask the patient what the number on the plate is. 8% of males and <1% of females are red green colourblind. |
| What are the differential diagnoses for a swollen optic disc? | Optic neuritis, papilloedema (must be bilateral), malignant hypertension, arteritic anterior ischaemic optic neuropathy (AION), non-arteritic AION. |
| Describe the clinical features of optic neuritis. | The disc usually appears swollen with a blurred margin. HOWEVER if the inflammation of the optic nerve occurz further behind the disc, the disc will not be swollen. This would be called a retrobulbar neuritis. Cup and colour unaffected. Pt usually complains of blurred vision and an ache behind the eye, especially on movement of the eye. Central visual acuity will be slightly reduced, and there may be some para central scotoma or an enlarged blind spot. RAPD will be present and on questioning and testing the patient you may find they have red desaturated in the affected eye. May have other transient neurological symptoms, e.g. tingling, vision blurring worse with exercise etc. There is a risk of demyelination/MS, especially with a recurrence - need MRI. |
| What is the clinical picture with papilloedema? | Swelling of the optic discs due to increased intracranial pressure. Symptoms: headaches, transient blurring of vision. Signs: swollen discs, splinter haemorrhages at disc margin, and cotton wool spots. May also have exudates if it has been going for a while. There will be an enlarged blind spot but no other visual field defect in the early phase. If the increased ICP is not corrected, the optic nerve will become atrophic, and at this late stage a gradual constriction of vision will be seen. At this point the changes are irreversible. |
| In what situation could you get unilateral papilloedema? | The only situation in which this could be unilateral is if the patent developed optic atrophy in one eye before developing the increased ICP. This only occurs in a condition called Foster Kennedy syndrome, where a frontal meningioma compresses one optic nerve, rendering it atrophic, before becoming large enough to cause an increase in ICP. |
| What is Arteritic Anterior Ischaemic Optic Neuropathy? | Inflammation of the blood supply to the optic disc, causing infarction of the optic nerve. Either giant cell arteritis or temporal arteritis - the inflammation of the temporal aa causes occlusion of the vascular supply to the optic nerve, and the nerve infarcts. Before this happens, the patient will complain of temporal headaches, which may or may not be associated with jaw claudication (chewing). Also the pt may lose weight and have muscle aches. Some say the condition is similar to polymyalgia rheumatica. Visual loss in giant cell arteritis is sudden, due to inflammatory infarction of the posterior ciliary arteries. Raised ESR and CRP. Disc margin appears blurred, disc is pale, cup is obliterated from all the swelling. |
| What is the management of Arteritic AION? | Treatment with high dose oral steroids (1-1.5mg/kg) must be started urgently, as infarction is irreversible and the other eye may go 2-3 weeks after visual loss in the first eye. Keep taking high dose for at least 3 consecutive days, until the ESR starts dropping. Then slowly taper treatment over 2-3 weeks down to a maintenance dose. Can be treated as outpatient. Will need a temporal artery biopsy, as the treatment is long and may have side effects. Ideally take biopsy within a week. Treatment continues for at least 2 years. |
| What is non-arteritic AION? | Artery is swollen from non-inflammatory causes, usually atherosclerosis. This causes obliteration of the lumen of the posterior ciliary arteries - infarction. Disc swelling and visual impairment is usually not as severe as that seen in arteritic AION. Usually only half the disc infarcts - top or bottom. ESR to raised as not an inflammatory condition. 50% of these patients are hypertensive. Diabetes also a risk. Treat with low dose aspirin. |
| What is optic atrophy? | End stage eye disease. Associated with APD. Pallor of disc. Can be caused by anything which compresses the optic nerve or interferes with its blood supply. |
| What are the 6 extraocular muscles? | Superior rectus, superior oblique, medial rectus, inferior oblique, inferior rectus, lateral rectus. |
| What is the innervation of the extraocular muscles? | All supplied by the oculomotor nerve (CN III) apart from the superior oblique trochlear nerve CN IV) and the lateral rectus (abducens nerve VI). |
| What is the effect of a IIIrd nerve palsy? | Medial rectus, inferior rectus, superior rectus, inferior oblique, levator palpebri superioris and pupil are affected (will be larger than normal on the affected side). Superior oblique and lateral rectus spared. Eye points down and out (unopposed action of the lateral rectus abducting and the superior oblique depressing). Ptosis on affected side means you will have to lift the lid to see the position of the eye. Pupil will be dilated but no afferent pupillary defect. |
| What is the effect of a IVth nerve palsy | Superior oblique affected. The role of the superior oblique is to allow the eye to move slightly down and also to rotate the eye slightly in (intorsion). So in a 4th nerve palsy, the eye is unable to look down and in on the affected side. Hence, vertical diplopia most marked on looking down and in. Bilateral cases may occur with head injuries. When looking straight ahead, the affected eye will be slightly above the other. Can do the eye tilt test. When abducting affected eye, will look quite normal, but when adducting, the affected eye will look upwards. |
| What is the effect of a VIth nerve palsy | Abducens palsy = an inability to abduct. Eye may drift medially on affected side due to pull of medial rectus. |
| What is the effect of a VIIth nerve palsy | The facial nerve supplies the muscles of facial expression, and it is involved in the muscles that close the eye, therefore a facial palsy may cause exposure. This can lead to exposure keratitis and in severe cases corneal perforation. Test corneal sensation - if affected, more likely to develop ulceration and other problems. Also test for Bell's phenomenon - pt's eyeballs roll up when they close the eye - mechanism that protects our corneas when we sleep. This determines whether you will need to tape this pt's eyes shut when they are sleeping. |
| Name some pupillary defects. | APD/RAPD, Adie's pupil, Argyll Robertson pupil, third nerve palsy (efferent pupil defect), Horner's syndrome, Light-near dissociation. |
| Describe the pathway for the pupillary light reflex. | Light stimulates the photoreceptors - retinal ganglion cells, and a signal is transmitted to the pretectal nucleus. After that, the Edinger-Westphal nucleus on the same side AS WELL AS the one on the opposite side are stimulated. Then the efferent impulse is sent via the inferior division of CN III. Therefore, both pupils will constrict even when light is only shone in one eye. |
| Describe the pathway for the pupillary near reflex. | Your pupils both constrict when you try to look at something very near. The information is sent from the pre-striate cortex in area 19 to the Edinger-Westphal nuclei. Vision is not a pre-requisite for this reflex to occur - even patients who are blind will have this reflex. Instead it is the thought that you are looking at something close to you that triggers the action of area 19. The EWNs then send efferent signals via the inferior division of CN III to cause pupillary constriction. |
| What happens in an Afferent Pupillary Defect (APD)? | The afferent pathway is from the retina up until the EWN. But the term APD denotes a pathology with the retina or the optic nerve (that is, before the optic chiasm). |
| What happens in RAPD? | The input to one side is reduced, so the pupils will not constrict as well. Swinging lamp test - affected eye will be seen to dilate paradoxically. |
| What is the difference between APD and RAPD? | APD: No direct or consensual response. RAPD: Reduced light and consensual response. Pupil dilates on the swinging light test. |
| What is the efferent pathway to the pupils? | It runs from the EWN as the inferior division of the third cranial nerve to the intraocular muscles; the pupil and the ciliary body. If there is an efferent pupillary defect, that means there is pathology here meaning that the pupil is not constricting as well as it should. The pupil of the affected side is large and remains large regardless of where you shine the light, as it is not an afferent problem. |
| What is Horner's syndrome? | Lesion of the sympathetic pathway (goes from hypothalamus down the neck and back up carotid). Affected pupil is smaller than usual. Pupil inequality is more pronounced in the dark. patient may have neck scars, partial ptosis (Mullers muscle) and the eye may appear to be sunken in (apparent enophthalmos). |
| What are Argyll Robertson pupils? | Due to tertiary syphilis (neurosyphilis). Pupils often small and irregular, may be asymmetrical. Sluggish light reponse. Light near dissociation. Pt may be blind from optic atrophy. Usually seen in 60-70 year olds. |
| What are the two types of muscle in the iris? | Sphincter and dilator |
| What are the two types of muscle in the ciliary body? | Circular and longitudinal |
| What do the sphincter pupillae and dilator pupillae muscles respond to? | Sphinter pupillae muscle responds to an increase in light and contracts, constricting the pupil. Is under parasympathetic control. Dilator pupillae muscle is under sympathetic control. Thus, when presented with a threatening stimuli that activates the fight-or-flight response, this innervation contracts the muscle and dilates the iris, thus temporarily letting more light reach the retina. |
| What happens during the accommodation reflex? | There is convergence and constriction of the pupils. The ciliary body circular muscle constricts - the zonule relaxes and the lens becomes rounder and fatter. |
| What is anisocoria? | When the pupils are different sizes to each other. 10% of the population have physiological anisocoria - usually a difference in diameter of <1mm. If there is a difference of >1mm or a recent onset, it must be assumed to be pathological. |
| What effects do TCAs, opiates and phenylephrine have on the pupils? | TCAs dilate, opiates constrict, phenylephrine in decongestants dilates pupils. |
| Describe the pathway of the 1st order neuron in the pupillary CONSTRICTION reflex. | Retina -> Optic chiasm -> optic tract -> Pretectum (midbrain). |
| Describe the pathway of the 2nd order neuron in the pupillary reflex | Here the neurons split into two, and goes to the accessory occulomotor nucleus (Edinger-Westphal) on BOTH sides of the brain. |
| Describe the pathway of the 3rd order neurons in the pupillary reflex | Efferent pathway. 3rd order neurons travel along the parasympathetic fibres of the surface of CNIII to act on the pupillary constrictor muscles. NB: Because the pathway splits at the pretectum, the effect is seen in both eyes even if the input is only in one. |
| Describe the pathway of the 1st order neuron in the pupillary DILATATION reflex. | Posterior hypothalamus -> comes down to ciliocentral sinus of Budge. |
| Describe the pathway of the 2nd order neuron in the pupillary DILATATION reflex. | Cilio spinal centre of Budge -> up to level of C2 (superficial cervical ganglion of sympathetic chain). |
| Describe the pathway of the 3rd order neuron in the pupillary DILATATION reflex. | Post ganglionic fibres. C2 -> splits and innervates sweat glands of the face, a superficial branch also splits off to innervate the dilator pupillae muscles, then a more superior brance innervates the sweat glands of the forehead and Muller's muscle (smooth muscle of eyelid). |
| What is the pathway for the accommodation response? | Remains unclear. Seems to be initiated in supranuclear centres in frontal and occipital lobes, then into the Edinger-Westphal nucleus to the constrictor pupillae. |
| What are the features of Horner's syndrome? | Horner syndrome (Horner’s syndrome) results from an interruption of the sympathetic nerve supply to the eye and is characterized by the classic triad of miosis (ie, constricted pupil), partial ptosis, and loss of hemifacial sweating (ie, anhidrosis). May also see apparent enophthalmus, and pigment changes in the iris. If the patient has a painful neck, must rule out an internal carotid artery aneurysm - listen with the bell. If unsure, vascular USS. |
| What is the function of Muller's muscle? | The first 1-2mm of elevation of the eyelid in normal gaze is maintained by the Muller's muscle, under sympathetic control. |
| What are some causes of diplopia? | CNIII, IV and VI palsies. Myaesthenia gravis (will usually be bilateral but unequal). Thyroid disease. |
| What must you check if there is a painful third nerve palsy? | Need to rule out posterior communicating artery aneurysm with a CT angiogram. |
| What is a sign of a carotid-cavernous fistula? | There will be a characteristic dilated, corkscrew pattern of blood vessels on the front of the eye. Usually clinically easy to tell if the problem is in the cavernous sinus as there will also be problems with the maxillary and ophthalmic divisions of the trigeminal nerve. |
| Describe the features of a vascular CNIII palsy. | Pupil is usually spared. Self-limiting. Due to HTN or DM - occlusion in vasa nervorum. Opening of pre-existing collaterals reduce the impact of the occlusion - this is why these palsies are self-limiting. The pupil is spared because they are in the parasymp bit of CNIII which has the pia mater blood supply for when the vasa nervorum part of CNIII is blocked. |
| What is the management of a vascular third nerve palsy? | Watch and wait. Get better blood glucose control. See every 2 weeks to review. If the pupils are ever involved, get imaging. |
| What is "Adie pupil"? | Enlarged pupil. "Tonic pupil" - absent direct and consensual light reflex and slow accommodation response. My be associated with reduced tendon reflexes (Holmes-Adie syndrome). Most often affects young women. Flu-like prodrome. Commonly seen in conjunction with HZO. |
| What is traumatic mydriasis? | Sequel of blunt trauma. Damage to the iris sphincter muscle. After trauma has resolved, the patient still has dilated pupil. If there is a large hyphaema, must drain, as the haem stains the cornea. When vessels rupture, sphincter muscle remains ischaemic - dilator muscle is unopposed. Cosmetic problems - when there is glare the eye waters and aches. |
| What is the management of traumatic mydriasis? | Can try drops to block the action of the dilator muscle (doesn't really work). Then try contact lenses with iris printed on them to prevent too much light entering the eye. |
| What is posterior synechiae? | There is a hypopyon (caused by corneal ulcers, severe anterior uveitis, post-op endophthalmitis or an intraocular tumour- rare) following intraocular inflammation. There is leakage of vessels forming the blood-aqueous barrier - forming a "glue" which causes adhesions of the iris pigment epithelium to the lens. |
| What is the management of posterior synechiae? | Topical steroids to treat the inflammation. Also prescribe mydriatic drops as this will stop the pain (cyclopentolate is shortest acting, homatropine is longer acting, atropine no longer used). When resolved, previous posterior synechiae can be a cause of anisocoria. |
| Describe the two types of optic neuritis. | Optic neuritis causes an RAPD. 2 types: Papillitis (inflammation of the disc): Blurrung of disc margin is seen. Acute retrobulbar neuritis (majority): Retina looks completely normal - but patient will complain of loss of vision of 6/6 to hand movements over a few days. In optic neuritis the rate of conduction in the optic nerve is slowed down - if you leave the light for longer on the affected pupil - give it more time for afferent fibres to conduct - will see constriction eventually. |
| What are some differentials for anisocoria where the smaller eye is the abnormal one? | Horner's (might have had ptosis corrected), posterior synechiae, pharmacological. |
| What lies in the inner third of the retina? | This is the ganglion cell layer - cell bodies then axons are laid out in an arcuate pattern. |
| What is the normal diameter of the optic disc? | 1.2-2.2mm diameter. Anything less is a hypoplastic disc. When it comes out behind the eye it is myelinated which doubles the vertical diameter. |
| The two optic nerves go back medially and confront each other above the sphenoid bone. Then it is the optic chiasm and there is cross over. What happens next? | Immediately after the chiasm it goes to the lateral geniculate nucleus. Fibres rotate 90⁰ and spread out in this part of the pathway. This means that superior retinal fibres lie medially, inferior fibres lie laterally by the time they reach the lateral geniculate body. |
| What happens as the fibres from the optic nerve leave the lateral geniculate body? | As the fibres want to continue their journey, the inferior fibres (now lying laterally) encounter the temporal horns of the lateral ventricles. This forces these fibres to go around these lakes of CSF - temporarily going into the temporal lobe. The superior fibres (now lying medially) travel on their own through the parietal lobe, after which they are rejoined by the estranged inferior fibres. The fibres then rotate back into their original formation now in the geniculate-calculine tract. They continue this way until they are in the visual cortex in the occipital lobe. |
| In the occipital lobe the optic nerve fibres are segregated again, how does this happen? | Macular fibres go to the medial tip of the visual cortex (on either side). The whole area of the visual cortex is supplied by the posterior cerebral artery, but the medial tip has a second source of perfusion by a small branch of the middle cerebral artery - so the macular fibres are sat in the "1st class lounge" of the visual cortex. |
| Describe the optic chiasm and its anatomical landmarks that could contribute to problems. | Above the sphenoid bone there is the sella turcica (lying under the optic chiasm). 20% of the time, the pituitary is slightly anterior/posterior to the optic chiasm, but still in pituitary plane. In 80% of cases they are fixated in the same plane. Above the optic chiasm is "Rathke's pouch" - this contributes to the development of the pituitary embryologically, and sits back as a pouch covered by meninges. This means either the pituitary could come up or Rathke's pouch could come down to compress the optic chiasm. A prolactinoma is most common in young women - usually benign but could destroy optic chiasm. |
| Describe the presentation and cause of a BITEMPORAL HEMIANOPIA. | Lesion is in optic chiasm - only place where both nasal fibres could be affected at the same time. Nasal retinal fibres are cut off therefore bitemporal vision is lost. Uncommon presentation - usually will have diagnosed and treated (usually with bromocriptine for pituitary tumours) before this stage. More often presents as a bitemporal superior or inferior quadrantonopia. |
| Describe the presentation and cause of a LEFT INCONGRUOUS HEMIANOPIA. | This is an optic tract lesion. Loss of the right hald of both retinas - so have lost left side of vision in both eyes. If it is not a similar/complete defect in each eye then it is called incongruous. A lesion that is retro-chiasmal will always affect one side of the visual field in both eyes (nasal in one, temporal in another). |
| Describe the presentation and cause of a LEFT HOMONYMOUS HEMIANOPIA. | This is caused by a retro-chiasmal lesion. 89-91% of the time, lesions in the optic tract produce an incongruous hemianopia. 89-91% of the time, lesions in the geniculate-calculine tract produce a homonymous hemianopia. As a general rule, the further away from the optic chiasm, the more EQUAL visual field loss becomes. It is related to the arrangement of the fibres and the type of insult - compression is more likely further forward (so some fibres may escape this) and vascular lesions are more likely further back. |
| Describe the presentation and cause of a LEFT HOMONYMOUS HEMIANOPIA WITH MACULAR SPARING. | This is due to a visual cortec CVA, as the macular fibres are spared in a posterior cerebral artery CVA as they are supplied by a branch of the MCA. |
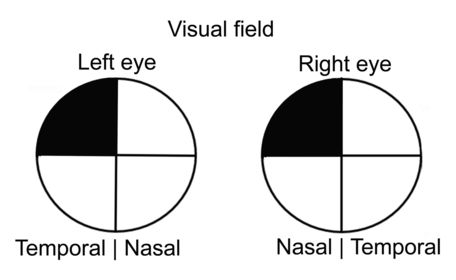
| Describe the presentation and cause of a LEFT SUPERIOR QUADRANTANOPIA. | This is due to a temporal lobe lesion. Inferior retinal fibres split off and go through the temporal lobe, and if they are cut off for some reason, a superior quadrantnopia is seen. A lesion in the right temporal lobe would lead to a left sided visual field loss. |
| Describe the presentation and cause of a LEFT INFERIOR QUADRANTANOPIA. | This is due to a parietal lobe lesion. Superior retinal fibres go through the parietal lobe - if there is a lesion there then that gives an inferior quadrantanopia. |
| How are visual fields formally tested? | With perimetry. Classed as static or kinetic depending on the type of machines used - kinetic is preferable. Mostly assessed for screening and monitoring of glaucoma. In most of the UK, only assess inner 30⁰ of vision - gives you enough clinical information. |
| Describe the visual field loss seen in glaucoma. | The field loss will cross the vertical midline but will respect the horizontal midline. Other defects (previously mentioned) won't cross the vertical midline - these need to be dealt with urgently. |
| Describe the visual field loss seen in retinitis pigmentosa. | Another cause of visual field loss - loss is from concentric, progressive loss of photoreceptors. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quer criar seus próprios Flashcards gratuitos com GoConqr? Saiba mais.